01 July 2025
Stress and Perimenopause: Why Your Nervous System Is on High Alert

Reading time 16 min

Reading time 16 min
You’ve handled pressure your entire career: tight deadlines, difficult coworkers, and performance reviews that didn’t go your way. Your nervous system took it all in stride, recovered, and kept moving. But over the last year or two, you feel yourself changing. Interestingly, it’s not the “big” stuff that tips the scales; you still handle those major challenges. Instead, it’s the ordinary friction: a colleague’s snide remark, a meeting that runs late, or an email that arrives at the wrong time. Your reactions feel disproportionate to the actual situation, and you notice the gap between the person you know yourself to be and how you are actually responding.
I’m not here to talk about “anxiety” or “burnout.” Instead, we’re going to look at a measurable shift in the neurobiological systems that govern how you process and recover from stress. Understanding the biology behind stress and perimenopause and what the evidence actually says about its effects is far more useful than any generic advice on how to “manage the pressure.”


You have two stress systems, and perimenopause affects them both.¹ This is why stress feels qualitatively different now from what you knew earlier in your career. Stress and menopause affect both the fast “fight-or-flight” response and the slower cortisol recovery system.
The first system is fast. The sympathetic-adreno-medullary (SAM) system operates within seconds of a perceived threat by:
This is your immediate fight-or-flight response. Think of it as the gas pedal, and think of estrogen as the mechanism that kept it from pressing down quite so hard.
The second system is slower. The hypothalamic-pituitary-adrenal (HPA) axis governs the sustained stress response. When a stressor registers, the hypothalamus signals the pituitary, which signals the adrenal glands to release cortisol. Cortisol helps sustain the stress response for minutes to hours, mobilizing energy and keeping you alert. When the stressor passes, rising cortisol feeds back to the hypothalamus and hippocampus to shut the cascade down. Fire, respond, recover. The system is designed to be self-limiting. In perimenopause, that last step stops working reliably.1
These two systems co-activate but serve different functions. SAM handles the immediate alarm. The HPA axis manages sustained response and recovery. In a well-regulated nervous system, they work in sequence. During perimenopause, the recovery half of that sequence degrades in both systems at the same time.
Before perimenopause, estrogen acted like a natural buffer for your heart and blood vessels. It helped keep your blood vessels relaxed and prevented your blood pressure from spiking too high when you were stressed or dealing with an adrenaline rush. Essentially, it kept your body’s “fight or flight” system from overreacting. As your estrogen levels drop, you lose that protective shield. Without it, your body’s physical response to stress becomes more intense and harder to control. One reason stress and perimenopause feel so intense is that estrogen previously acted as a buffer against nervous system overactivation.
Research shows that after menopause, the part of your nervous system responsible for “fight or flight” is much more active, nearly three times higher than in younger women, even when you’re just resting.2 When something stressful happens, your blood pressure spikes higher and takes a lot longer to come back down. It’s like your body is hitting the gas pedal harder while the brakes are getting weaker.3 The “wired” feeling lasting all evening, the clenched jaw, or lying in bed at night unable to relax isn’t because you’re overreacting. It is a physical state called sympathetic overdrive. Your body is stuck in high gear and simply doesn’t have the tools to reset itself like it used to.
The HPA axis has a critical calming mechanism that rarely gets discussed. In the brain, progesterone is converted into a compound called allopregnanolone. This compound activates GABA receptors, which are the brain’s main “off switch” for stress. These are the same receptors that anti-anxiety medications target to help you relax. Think of it as your brain’s natural brake fluid. When allopregnanolone is working, it helps slow down your stress response and keeps your system from redlining.1
As progesterone drops during perimenopause, allopregnanolone falls with it. The brain loses its endogenous calming signal when its stress machinery is becoming less regulated. The HPA axis becomes much more sensitive. It triggers faster, releases higher levels of cortisol, and takes a lot longer to finally turn off.1
This cortisol disruption usually follows a few familiar patterns. Some women have high cortisol all day long, which is just a sign of the physical strain on their bodies. Others have high cortisol at night, creating that “wired-but-tired” feeling: you’re wide awake at midnight but completely exhausted by morning. Both of these patterns ruin your sleep, and poor sleep makes every other symptom worse. Research shows that cortisol levels rise significantly during the transition to menopause, and this is caused by hormonal changes, not just the stress of daily life.2
Curious Fact. Allopregnanolone is so important for mood and brain function that a synthetic version was created as the first drug specifically to treat postpartum depression. The same chemical pathway that shifts so drastically after childbirth also changes during perimenopause. This change is likely why many women feel more vulnerable to mood swings and anxiety during this time. Despite this clear connection, the parallel between postpartum and perimenopause is almost never discussed with patients.
The prefrontal cortex acts like your brain’s “manager.” It’s responsible for keeping your cool under pressure, making smart decisions, and regulating your emotions. When your “fear center” (the amygdala) sends out an alarm, the prefrontal cortex uses logic to calm things down. For example, if someone criticizes you in a meeting, this part of the brain helps you stay professional and strategic instead of getting defensive. Estrogen supports this circuit directly: it maintains the chemical signaling between the prefrontal cortex and amygdala allowing your logical brain to stay in control of your emotional reactions.4
As estrogen levels drop and fluctuate, your “alarm center” (the amygdala) becomes more sensitive, while your logical brain (the prefrontal cortex) loses its ability to keep it in check. Brain scans show that in perimenopause, the amygdala can become stuck in a “high alert” mode.5 Because the logical part of your brain can’t dial it back as easily, you might go from perfectly calm to furious in three seconds and then feel confused about why you reacted so strongly. One study found that using an estrogen patch for just three weeks helped quiet this overactive circuit and improved symptoms.5
Brain glucose metabolism drops measurably in the regions responsible for emotional control, memory, and higher-order thinking. Mosconi’s neuroimaging work found up to a 30% reduction in glucose metabolism in these regions in midlife women, a deficit not seen in age-matched men.6 The prefrontal cortex, already losing hormonal support for its signaling, is also losing fuel. It’s two different problems hitting the same system at once.
Hormonal shifts affect three of your brain’s key chemical systems all at once.7
These three systems don’t change one by one; they change at the same time. That’s why the mood swings, the constant low-level anxiety, and the days when you just can’t get started can affect you at the same time. It feels like one big problem, but it’s actually three different systems losing their balance simultaneously.
Underlying all of this is a mechanism that amplifies the rest. Estrogen keeps the brain’s immune cells, called microglia, in a protective, anti-inflammatory state.8 When estrogen withdraws, microglia shift toward a pro-inflammatory state in the amygdala, hippocampus, and prefrontal cortex – the three regions most central to stress regulation, emotional response, and memory.8 This neuroinflammation makes it harder for your brain cells to communicate and makes them less resilient.
This creates a self-repeating loop: constant stress makes the inflammation worse, and an inflamed brain is less capable of handling stress. On top of that, high cortisol levels lower a protein called BDNF, which acts like “Miracle-Gro” for your brain. Without enough BDNF, your brain loses its ability to bounce back and recover fast from emotional strain.9,10
Research consistently shows that perimenopausal women, not postmenopausal women, report the highest levels of perceived stress, anxiety, and feeling “on edge.” Women who have completed the transition and reached stable (even if lower) estrogen levels report better stress tolerance than those still in the fluctuation. The intensity peaks at perimenopause and comes back down.11
The primary driver of that peak is not how low estrogen drops. It is how unpredictably it fluctuates.12
Week-to-week variability in estrogen levels predicts depression and emotional sensitivity to rejection far more strongly than absolute estrogen levels.12 Women whose estrogen levels fluctuate dramatically tend to have stronger reactions to stress. They feel social rejection more deeply and take much longer to recover emotionally after something upsets them. Stable hormones, even at a lower postmenopausal baseline, allow the brain’s fear and stress circuits to re-adapt. The chaos of perimenopause itself is neurologically harder than the quiet that follows it.
Women who have a history of anxiety or trauma often face extra challenges during this phase. When fluctuating estrogen levels make the brain’s “alarm center” amygdala more reactive, a nervous system that used to stay under control starts to struggle. Perimenopause doesn’t necessarily create these issues, instead, it tends to unmask vulnerabilities that were already there.13
When you run your stress systems on high alert for too long without enough recovery, it creates what researchers call allostatic load. This is essentially the physical wear and tear on your body from constantly trying to adapt to stress. When your stress response triggers but never fully resets, the system starts to break down. Your cortisol patterns get flatten, your brain’s “off switch” stops working well, and your ability to manage stress naturally disappears. This isn’t a sign of weakness. It is a predictable biological result of being “on” all the time without the chance to properly recover.
The impact of brain changes is very specific, and it affects the exact skills you need for a senior professional role. Chronic stress and menopause together create a much heavier cognitive load than either one alone.
Think of your brain’s capacity as a glass. Before perimenopause, your daily routine might have filled that glass halfway by the time you got to work. Now, because of hormonal changes, anxiety and poor sleep, the glass is already nearly full before your day even starts. When a complex question comes up in a meeting, there’s simply no room left for deep thinking. Your “glass” didn’t get smaller; the baseline demands just got much higher.
Many professional women notice this first when they struggle to find the right word. In neuroscience, this is called the “tip-of-the-tongue” state. You know the meaning and could describe the concept, but the actual word is stuck. This usually gets worse when you feel like you’re being watched or judged, the exact moments when you need to be most articulate. Dealing with perimenopause while under professional pressure means your brain is working under two major constraints that most other people in the room don’t have to deal with.
There is also a shift in how you process your surroundings. Estrogen helps your brain filter out background noise. As it fluctuates, that filter weakens. An open-plan office that used to be fine might suddenly feel intolerable: the overhead lights feel too bright, the sound of someone typing becomes a distraction, and the room temperature is impossible to ignore. This isn’t a personality change; it’s a physical change in how your brain handles sensory input while your stress system is already running hot.10
The data shows one very important thing: these changes affect your speed and access, not your actual intelligence. Your brain might process things a little slower or take longer to find a piece of information under pressure. However, your ability to reason, use strategic judgment, and make complex decisions remains intact. For most women, brain function returns to its normal baseline once they are through menopause.
Signs Your Nervous System Is Dysregulated During Perimenopause
Perimenopause is defined by fluctuating estrogen and falling progesterone. These hormones normally help manage the brain circuits, including the amygdala and prefrontal cortex, that identify threats and control your stress response. As these hormones become unstable, the same everyday stressors can trigger a larger reaction in the brain and cause cortisol levels to stay higher for longer than they used to.
At a biological level, your nervous system shifts into a state of “high alert.” This means a higher baseline of tension, an easier startle response, and a faster jump into fight-or-flight mode without the usual “braking” system to calm you down. In everyday life, this shows up as increased irritability, feeling easily overwhelmed, and lower resilience to daily hassle, essentially, your capacity to handle physical and emotional stress becomes much smaller.22
In normal conditions, cortisol follows a steady daily cycle: it is low at night, peaks in the morning to help you wake up, and gradually drops throughout the day. During perimenopause, this rhythm becomes erratic. Studies show weaker morning peaks and higher levels in the evening or at night, especially for those dealing with broken sleep.
This creates a contradictory state where you feel exhausted from poor sleep, yet your body remains physically “wired” due to high cortisol. In the brain, falling progesterone reduces the chemicals that help you relax, while fluctuating estrogen disrupts the signals that manage mood and alertness. This weakens your ability to calm down, making it hard to “turn off” even when you feel completely spent.22
The drop in estrogen during perimenopause is linked to increased muscle tension and a lower threshold for pain, particularly in the jaw and facial muscles. This hormonal change, combined with higher anxiety and poor sleep, makes it more likely that you will grind your teeth at night or clench your jaw during the day as your stress system stays stuck in “high gear.”
From the perspective of your nervous system, jaw tension is a physical sign that your body is staying in a state of high alert. These muscles remain partially tensed even when you are resting. Over time, this constant tension creates a feedback loop: the resulting headaches and facial pain signal to your brain that you are under stress, further reinforcing the feeling that your body can never fully switch off.
Estrogen helps the brain filter and manage sensory information. As levels fluctuate and drop, your sensitivity to light, sound, touch, and smell can increase, meaning the same environment creates a much stronger reaction in the brain. This is why ordinary settings, like a noisy store or a crowded office, can suddenly feel overwhelming and trigger an urgent need to escape.
Biologically, this happens because the brain’s emotional centers are more reactive, while the “filters” that usually block out distractions are weakened by stress and lack of sleep. Because your nervous system is already on high alert, it reaches its breaking point much faster. Poor sleep further drains your brain’s energy, leaving it with less capacity to ignore irrelevant noise and making everything feel louder and more intense.
Menopause is caused by the natural depletion of eggs in the ovaries. There is no proof that psychological stress “causes” menopause in a direct way, and saying so would be inaccurate.
However, the evidence shows a more complex connection. High levels of stress, fewer financial resources, and difficult life events are linked to starting menopause earlier, sometimes before age 45. While we don’t fully understand the “why” yet, research shows that women carrying a heavy “stress load,” especially those with histories of trauma or financial hardship, often start the transition sooner and experience more severe symptoms.14
What we do know for sure is that stress and menopause symptoms feed into each other once the transition begins.11,12 For example:
Chronic stress is one of the biggest factors we can change to help manage how long and how intense menopause symptoms last. This is why addressing stress isn’t just about “feeling better”; it’s a key part of managing your physical health during this transition.
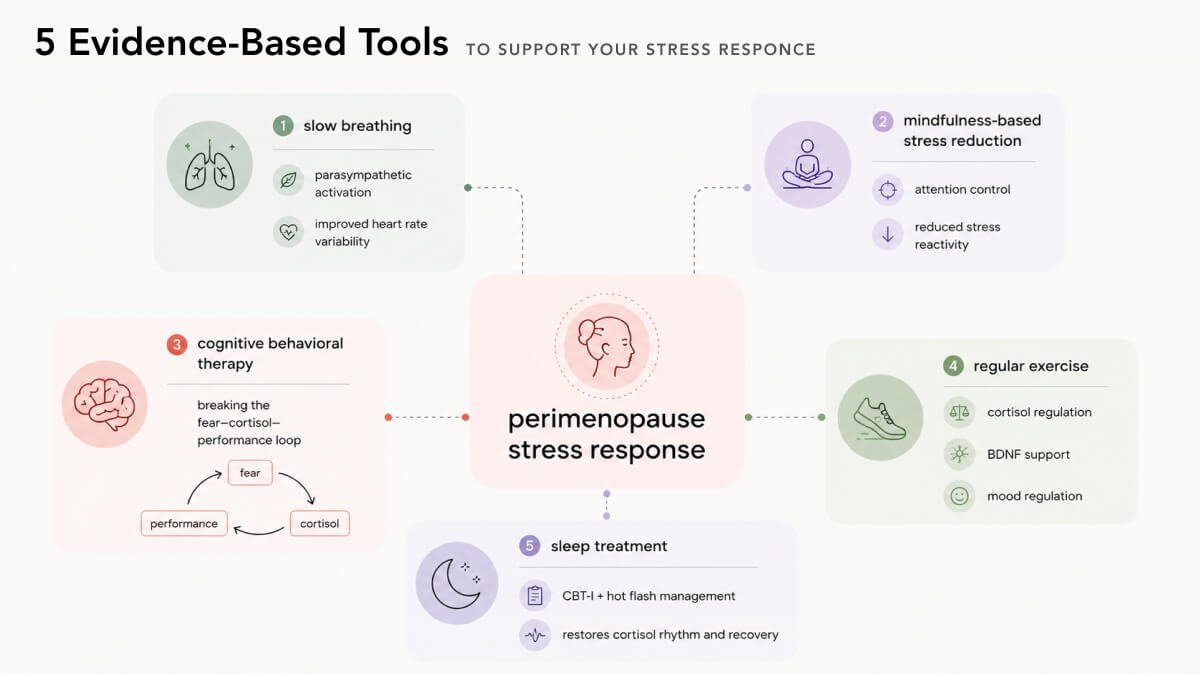
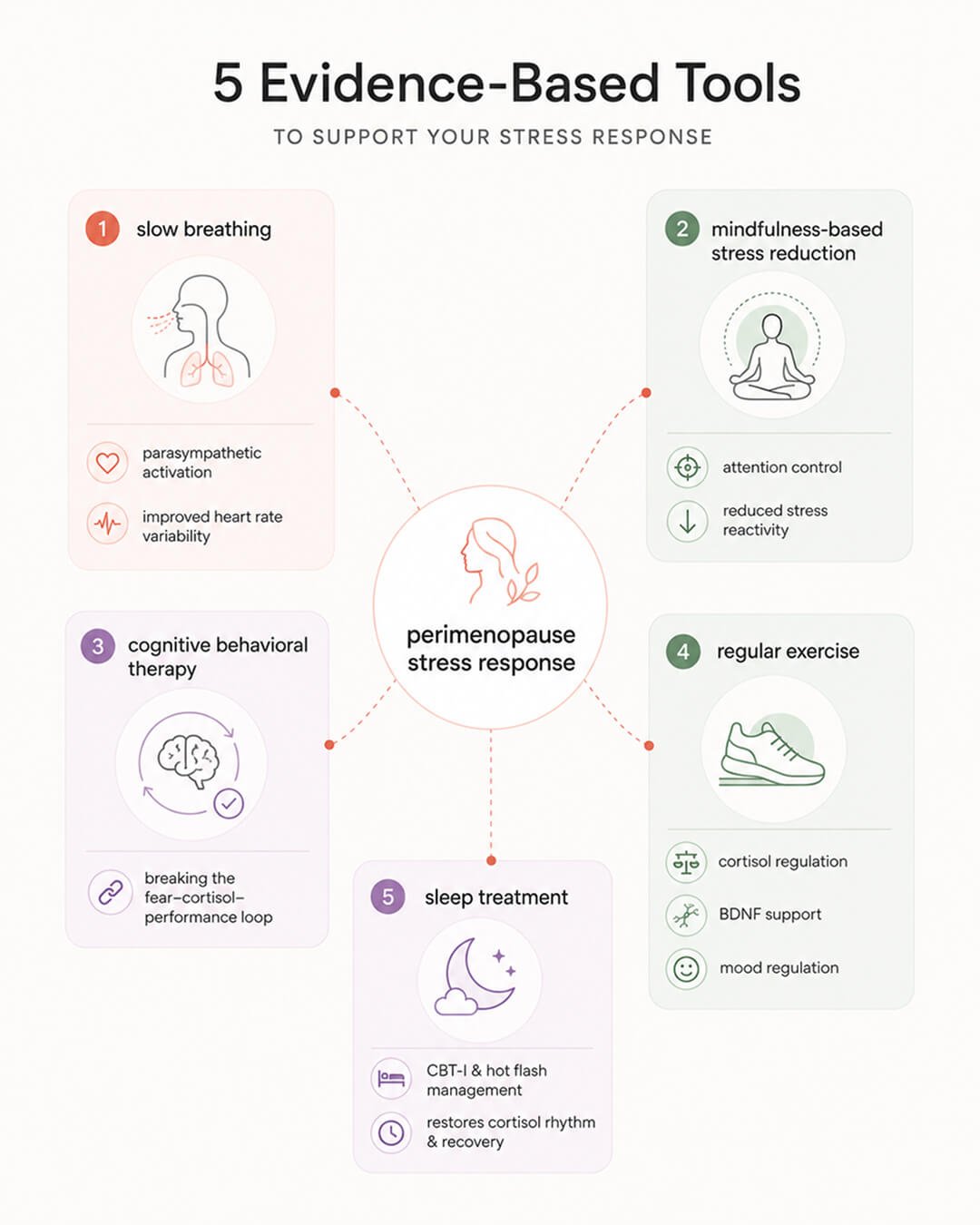
Slowing your breathing to about six breaths per minute (with your exhales slightly longer than your inhales) directly triggers your body’s “off switch.” This is a physical way to activate the parasympathetic nervous system, which acts as a counterweight to the “fight or flight” surge. At this pace, your breathing and heart rate sync up in a way that improves your heart rate variability, which is a key sign of a healthy, resilient nervous system. Research shows that regular practice (daily for 15 minutes) can lower your blood pressure and significantly reduce how much stress you feel.15
For professional women in high-pressure roles, this is a practical tool. Spending 8-10 minutes on slow, paced breathing before a presentation or a tough meeting can stop the cortisol spike that usually impairs with your memory and your ability to find the right words. It’s a mechanical reset for your brain that takes effect in minutes and only requires a moment of quiet before you walk into the room.
Mindfulness-Based Stress Reduction (MBSR) is a structured eight-week program that has been used in clinics since 1979. It’s a secular approach that uses meditation, body scans, and gentle movement to help manage stress. In a rigorous randomized controlled trial specifically in perimenopausal women, the program significantly lowered stress, anxiety, and depression while improving sleep. The biggest improvements were seen in women who already struggled with their mood or were especially sensitive to hormonal changes.16 A meta-analysis of 13 different studies confirmed these results, showing that mindfulness consistently helps women during the menopause transition.17 Mindfulness-based approaches are increasingly recommended for stress and menopause because they directly improve nervous system regulation.
For professional women, the main benefit of MBSR is that it trains your brain to control where it puts its attention. It teaches your “logical brain” (the prefrontal cortex) how to stop negative or anxious thoughts before they spiral and drain your mental energy. This is exactly the cycle that usually leads to “brain fog” or feeling overwhelmed during a busy workday. Because these skills help you stay focused under pressure, this training is now widely used in high-stakes professional environments.
Cognitive Behavioral Therapy (CBT) helps you break the thought patterns that keep your stress levels high. During perimenopause, many professional women get stuck in a specific loop: the fear of “blanking out” in a meeting raises your cortisol, which actually makes it harder to find the right words, which then confirms your fear and spikes your cortisol even more. CBT gives you practical tools to catch and stop that spiral before it ruins your day.
In clinical trials, CBT tailored for perimenopause has been shown to reduce anxiety, improve quality of life, and even lessen physical symptoms.¹⁸ Other studies have found that it consistently helps with depression, sleep problems, and how much hot flashes interfere with daily life. These benefits usually lasted long after the sessions ended.19,20 The best part is that these programs are structured and efficient. For menopause symptoms, they typically involve about eight sessions rather than years of therapy.
Regular aerobic exercise at a moderate intensity is one of the best ways to keep your cortisol levels in check. This means “Zone 2” exercise (a pace where you can still hold a conversation) for 45 minutes or more. This type of movement helps your stress system stay balanced, boosts the “growth juice” protein (BDNF) that drops when estrogen levels fall, and supports your mood-regulating chemicals like dopamine and serotonin, all without adding more stress to your body.9
However, there is an important warning for women who are already feeling burnt out: too much high-intensity training (like heavy HIIT or sprints) can actually overload an already strained system. This can lead to more fatigue, worse sleep, and even increased belly fat. Medical experts recommend keeping high-intensity sessions to just once or twice a week. The rest of your routine should be built on moderate aerobic work (at least 150 minutes a week) and strength training two to four times a week.
None of these strategies will work at their best if your sleep is constantly interrupted.
Research has found that broken sleep, not just the drop in estrogen, is what really throws your stress system out of balance. It causes your cortisol to stay high at bedtime and ruins the natural morning boost you need to start your day regulated. Sleep isn’t just one item on a checklist; it’s the foundation. If you fix your sleep, your cortisol levels will often follow.²¹ For perimenopausal sleep issues, Cognitive Behavioral Therapy for Insomnia (CBT-I) has the strongest evidence for success. It works better and lasts longer than basic “sleep hygiene” tips or melatonin.
If hot flashes are what keep waking you up, the most direct first step is talking to a doctor about Hormone Replacement Therapy (HRT). Stabilizing your body temperature often fixes your sleep before you even need to try other treatments.
I know what it’s like to sit in a meeting, feel an overreaction bubbling up, and have to fight to keep it inside. You manage it. You don’t say the wrong thing. But afterward, you dwell on it much longer than you should, and you find yourself constantly monitoring your own behavior in a way you never had to before.
Your brain isn’t failing. Stress and perimenopause change how the nervous system regulates emotional recovery, cortisol, and cognitive performance.
It is trying to regulate itself while its main signaling tool has become unreliable, and every system it uses to manage stress has changed at the same time. The strategies with the strongest evidence aren’t just “relaxation techniques.” They are precision tools designed to fix specific physical mechanisms. That distinction is vital when you need your brain to perform at its best.
Dr. Jūra Lašas
1.
Gordon, J. et al. Ovarian hormone fluctuation, neurosteroids, and HPA axis dysregulation in perimenopausal depression: a novel heuristic model (2015). https://doi.org/10.1176/appi.ajp.2014.14070918
2.
Klassen, S. A. et al. The impact of ageing and sex on sympathetic neurocirculatory regulation (2021). https://doi.org/10.1016/j.semcdb.2021.01.001
3.
Wenner, M. M. et al. Influence of Age and Estradiol on Sympathetic Nerve Activity Responses to Exercise in Women (2022). https://doi.org/10.1249/MSS.0000000000002823
4.
Yap, S. et al. Decreased Medial Prefrontal Cortex Glutamate Levels in Perimenopausal Women (2021). https://doi.org/10.3389/fpsyt.2021.763562
5.
Hynd, M. et al. Estradiol modulates resting-state connectivity in perimenopausal depression (2024). https://doi.org/10.1016/j.jad.2024.11.068
6.
Mosconi, L. et al. Menopause impacts human brain structure, connectivity, energy metabolism, and amyloid-beta deposition (2021). https://doi.org/10.1038/s41598-021-90084-y
7.
Barth, C. et al. Sex hormones affect neurotransmitters and shape the adult female brain during hormonal transition periods (2015). https://doi.org/10.3389/fnins.2015.00037
8.
Vegeto, E. et al. Estrogen anti-inflammatory activity in brain: a therapeutic opportunity for menopause and neurodegenerative diseases (2008). https://doi.org/10.1016/j.yfrne.2008.04.001
9.
Kim, B. et al. Regular Leisure-Time Physical Activity is Effective in Boosting Neurotrophic Factors and Alleviating Menopause Symptoms (2020). https://doi.org/10.3390/ijerph17228624
10.
Mosconi, L. et al. In vivo brain estrogen receptor density by neuroendocrine aging and relationships with cognition and symptomatology (2024). https://doi.org/10.1038/s41598-024-62820-7
11.
Kuck, M. J. & Hogervorst, E. Stress, depression, and anxiety: psychological complaints across menopausal stages (2024). https://doi.org/10.3389/fpsyt.2024.1323743
12.
Gordon, J. et al. Estradiol variability, stressful life events, and the emergence of depressive symptomatology during the menopausal transition (2016). https://doi.org/10.1097/gme.0000000000000528
13.
Lozza-Fiacco, S. et al. Baseline anxiety-sensitivity to estradiol fluctuations predicts anxiety symptom response to transdermal estradiol treatment in perimenopausal women (2022). https://doi.org/10.1016/j.psyneuen.2022.105851
14.
Blackson, E. A. et al. Experiences of menopausal transition among populations exposed to chronic psychosocial stress in the United States: a scoping review (2024). https://doi.org/10.1186/s12905-024-03329-z
15.
Sévoz-Couche, C. & Laborde, S. Heart rate variability and slow-paced breathing: when coherence meets resonance (2022). https://doi.org/10.1016/j.neubiorev.2022.104576
16.
Gordon, J. et al. Endocrine and psychosocial moderators of mindfulness-based stress reduction for the prevention of perimenopausal depressive symptoms: A randomized controlled trial (2021). https://doi.org/10.1016/j.psyneuen.2021.105277
17.
Liu, H. et al. The effects of mindfulness-based interventions on anxiety, depression, stress, and mindfulness in menopausal women: A systematic review and meta-analysis (2023). https://doi.org/10.3389/fpubh.2022.1045642
18.
Kim, D. S. et al. Efficacy of cognitive behavioral therapy for menopausal symptoms and quality of life in Korean perimenopausal women: A pilot randomized controlled trial (2024). https://doi.org/10.1016/j.maturitas.2024.108103
19.
Spector, A. et al. The effectiveness of psychosocial interventions on non-physiological symptoms of menopause: A systematic review and meta-analysis (2024). https://doi.org/10.1016/j.jad.2024.02.048
20.
Green, S. M. et al. Cognitive behavior therapy for menopausal symptoms (CBT-Meno): a randomized controlled trial (2019). https://doi.org/10.1097/gme.0000000000001363
21.
Cohn, A. Y. et al. Effects of Sleep Fragmentation and Estradiol Decline on Cortisol in a Human Experimental Model of Menopause (2023). https://doi.org/10.1210/clinem/dgad285
22.
Pillerová, M. et al. Molecular actions of sex hormones in the brain and their potential treatment use in anxiety disorders (2022). https://doi.org/10.3389/fpsyt.2022.972158

Healthy Body & Mind
Brain & Mind Wellness

Treatments & Supplements

Understanding Menopause

Scientific Research

Understanding Menopause

Lifestyle & Self-Care

Scientific Research

Eat to Thrive

Scientific Research

Treatments & Supplements

Understanding Menopause

Understanding Menopause
Understanding Menopause

Lifestyle & Self-Care
We use cookies and similar technologies to ensure the proper functioning of our website, personalize content, provide social media features, and analyze traffic. By clicking “I Agree”, you consent to the use of these technologies.
No results




