16 December 2025
Menopause Symptoms and Work Performance: Science-Backed Solutions

Reading time 12 min

Reading time 12 min
Menopause affects workplace performance for 65% of professional women, yet most navigate this transition in silence. If you experience perimenopause or menopause symptoms – brain fog, memory lapses, difficulty focusing in high-stakes meetings – you’re facing challenges that directly impact your career.
Research shows menopause symptoms genuinely affect work, particularly for women in leadership roles where cognitive demands are highest. The goal is to understand what menopause is doing to the brain in a work setting, apply strategies that are supported by real science, and make informed choices about managing this transition while maintaining professional credibility.
Manager training and brief CBT have the strongest evidence. Health education helps self management. Flexible schedules, short breaks, and better temperature control ease daily symptoms. Combine workplace adjustments with medical care to protect performance and retain talent.
First, let’s talk numbers. Over 80% of women experience menopausal symptoms, and about 25-40% say those symptoms make work genuinely more difficult. For some, it’s manageable. For others, it’s a daily struggle that affects everything from concentration to career choices1.
What’s surprising is which symptoms cause the most trouble at work. While hot flashes get a lot of attention (and yes, they’re disruptive), the real workplace culprits are often the invisible ones2,3:

A landmark Mayo Clinic study of 4,440 employed women aged 45-60 found that women with the most severe menopause symptoms were 15.6 times more likely to report an adverse work outcome (like missing work, cutting hours, or even quitting) compared to those with mild symptoms4.
Same study reported that missed workdays from menopause symptoms cost the US economy an estimated $1.8 billion in lost productivity every year (without taking into an account reduced hours, early retirements, or stepping back from leadership roles).
Let’s talk about the elephant in the room: menopause is still treated like a taboo topic at work. Many women are reluctant to disclose menopause-related difficulties to managers, often due to stigma or fear of being perceived as less capable. This is particularly true in male-dominated industries or for women in leadership positions where showing ‘weakness’ feels risky5.
“Most managers have received zero training about menopause.”
They may be sympathetic in theory but have no idea what practical support looks like. Without awareness and training, even well-meaning managers don’t know how to help – or that they should be helping at all.
Sometimes it’s the simple things that make symptoms unbearable: poor temperature control (try having a hot flash in a stuffy office), lack of rest areas, inflexible schedules that don’t allow for medical appointments or recovery from poor sleep. These environmental factors can turn manageable symptoms into workplace crises.
Women in leadership roles face unique challenges when navigating the menopause transition at work.
Higher cognitive demands: Executive function (the neuroscience term and the job requirement) handles planning, decision-making, working memory, and strategic thinking. Perimenopause disrupts these exact cognitive functions first.
Greater scrutiny: Memory lapses in a manager meeting are noticed. Forgetting details in a board presentation creates reputation risk. Slower processing in high-stakes negotiations matters.
Disclosure risks: Will symptoms affect your promotion? Will you be perceived as less capable? If you’ve spent years fighting for your seat at the table, will this give ammunition to people who already question whether women belong in leadership?
Research supports these concerns. A Mayo Clinic study found that women with the most severe menopausal symptoms were 15.6 times more likely to report negative work outcomes. These included reduced working hours, turning down promotions, and leaving the workforce earlier than planned.
For women in senior roles, this is not only about symptom management. It is about protecting careers that took decades to build.
A 2024 systematic review analyzed workplace menopause interventions to determine which have scientific support. The results are clear: some interventions have strong evidence, while others sound good but lack rigorous testing.
Here’s what separates proven strategies from wishful thinking:6,7,8
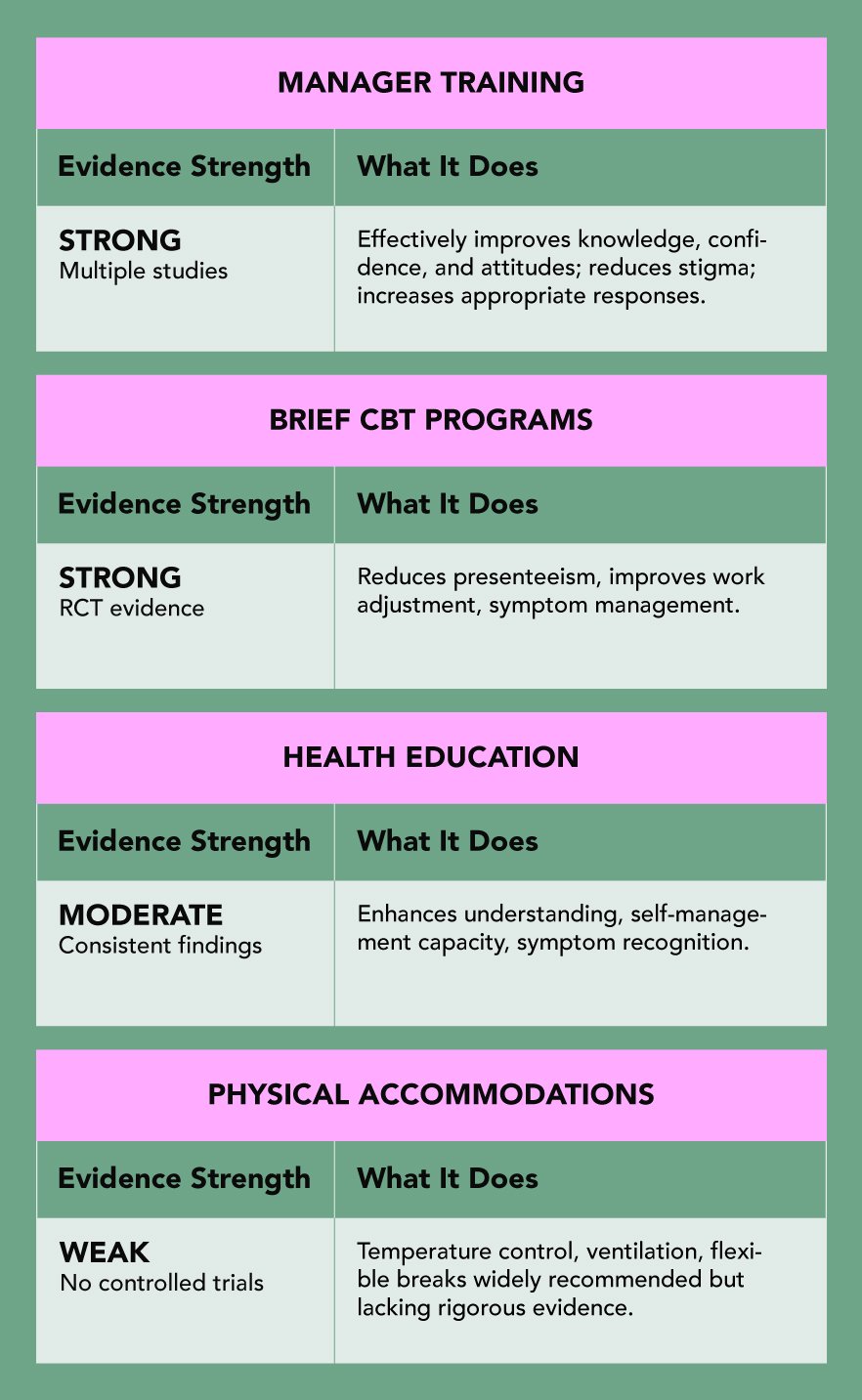
Manager training and brief CBT programs have the strongest research support. Workplace flexibility and environmental changes help symptom management, though evidence is less robust. Start with what works, not what’s trendy.
Although flexible work arrangements consistently emerge as highly valued by employees9. This includes:
These aren’t special favors – they’re reasonable accommodations that help retain experienced employees and prevent unnecessary workforce exits.
The cognitive changes many women notice at work are not imagined. They reflect measurable, temporary changes in brain systems involved in memory, focus, and executive function.
Brain imaging studies show that during perimenopause the brain goes through a period of reorganization.
Gray matter volume can temporarily decrease in the hippocampus, a region central to memory. Metabolic activity shifts in the prefrontal cortex, which supports planning, decision-making, and cognitive control. At the same time, patterns of neural connectivity change as the brain adapts to fluctuating hormone levels.
This is not cognitive decline. It is a transitional phase in how the brain functions under hormonal change.
Dr. Jūra Lašas


Research shows 65-80% of women experience menopause symptoms, and 25-40% report these symptoms make work genuinely more difficult. Cognitive symptoms (brain fog, memory issues, poor concentration) affect work performance most, particularly in roles requiring sustained focus and decision-making.
In the USA, menopause symptoms may qualify for ADA accommodations if they substantially limit major life activities. Reasonable accommodations might include flexible schedules, temperature control, quiet workspace, or reduced meeting density. Documentation from a healthcare provider helps.
There is no single right answer. This decision depends on your workplace culture, your relationship with your manager, and whether any adjustments would genuinely make a difference to how you function at work. Some women find that being open leads to practical support. Others choose to manage symptoms privately, and that can be just as valid. Regardless of what you decide, keeping a record of symptoms is useful. It supports medical care and gives you context if workplace conversations become necessary later on.
The strongest evidence supports manager training and brief cognitive behavioral therapy, particularly for symptom coping and work functioning. Flexible work arrangements can reduce symptom burden by allowing women to align demanding tasks with higher-energy periods. Environmental adjustments such as temperature control and access to quiet rest areas can meaningfully reduce discomfort during the workday. Health education also plays a role by improving symptom recognition and self-management. The best outcomes are seen when workplace strategies are combined with appropriate medical care rather than used in isolation.
For most women, cognitive symptoms are most noticeable during late perimenopause and the early postmenopausal years, roughly the two to five years surrounding the final menstrual period. This is when hormonal fluctuations are greatest and the brain is adapting in real time. For many, symptoms ease after menopause as the brain adjusts to a new hormonal baseline. That said, experiences vary widely. Severity, duration, job demands, sleep, stress, and access to treatment all influence how long symptoms affect work functioning.
1.
Safwan, N. et al. Menopause in the workplace: Challenges, impact, and next steps. (2024) https://doi.org/10.1016/j.maturitas.2024.107983
2.
Whiteley, J. et al. The Impact of Menopausal Symptoms on Quality of Life, Productivity, and Economic Outcomes. (2013) https://doi.org/10.1089/jwh.2012.3719
3.
O’Neill, M. et al. Impact of menopausal symptoms on work and careers: a cross-sectional study. (2023) https://doi.org/10.1093/occmed/kqad078
4.
Faubion, S. et al. Impact of Menopause Symptoms on Women in the Workplace. (2023) https://doi.org/10.1016/j.mayocp.2023.02.025
5.
Faubion, S. et al. Menopause and the workplace: consensus recommendations from The Menopause Society. (2024) https://doi.org/10.1097/GME.0000000000002415
6.
Jack, G. et al. Menopause in the workplace: What employers should be doing. (2016) https://doi.org/10.1016/j.maturitas.2015.12.006
7.
D’Angelo, S. et al. Impact of Menopausal Symptoms on Work: Findings from Women in the Health and Employment after Fifty (HEAF) Study. (2022) https://doi.org/10.3390/ijerph20010295
8.
Hardy, C. et al. Self-help cognitive behavior therapy for working women with problematic hot flushes and night sweats (MENOS@Work): a multicenter randomized controlled trial. (2018) https://doi.org/10.1097/gme.0000000000001048
9.
Potočnik, K. et al. Managing menopause transition in the workplace: The double-edged sword of flexible work. (2025) https://doi.org/10.1111/joop.70032
Eat to Thrive

Healthy Body & Mind
Brain & Mind Wellness

Treatments & Supplements

Eat to Thrive

Understanding Menopause

Scientific Research

Understanding Menopause

Eat to Thrive
Lifestyle & Self-Care
Scientific Research

Exercise & Nutrition

Eat to Thrive

Symptoms Explained

Eat to Thrive

Eat to Thrive

Scientific Research

Treatments & Supplements
We use cookies and similar technologies to ensure the proper functioning of our website, personalize content, provide social media features, and analyze traffic. By clicking “I Agree”, you consent to the use of these technologies.
No results

