10 June 2025
How to Tell If Menopause Health Advice Is Actually Science-Backed

Reading time 10 min

Reading time 10 min
Science. It’s a word that gets thrown around a lot, but what does it really mean? Understanding science basics for menopause health advice can help you navigate symptoms, treatments, and advice with real confidence. And it matters more than ever. Menopause misinformation is everywhere (in ads, in your feed, in conversations with friends), and most of it sounds persuasive. The question is no longer “is there information?” It’s “how do I tell what menopause health advice is actually science-backed?”
Women in perimenopause and menopause were underrepresented in clinical research for decades. For many of the symptoms we actually care about (brain fog, joint pain, mood shifts, libido), the number of large, well-conducted trials in menopausal women is still small. The science has not caught up with the lived reality.
This gap makes menopause health advice evidence harder to find and easier to distort.
Add a booming market. Industry analyses project the global menopause market will reach over $24 billion by 2030, with dietary supplements as the dominant and fastest-growing segment. We have questions about menopause health advice and science cannot yet answer all of them. That gap is the commercial opening.1
Finally, let’s also add the algorithm. A 2025 UK analysis of 180 top-ranked HRT claims across Facebook, Google, Instagram, TikTok, YouTube, and X found that 67% fell outside the indications listed by the British National Formulary and NICE guidance, and 77% came from a source with a conflict of interest.2 One of the journals put it bluntly: menopause misinformation is now harming care.3 This problem leads women toward unnecessary testing, unproven products, and sometimes away from treatments that actually work.
At its core, science is just a way to figure things out, reliably and systematically. Imagine you’re trying to figure out which moisturizer works best for your skin. You wouldn’t just pick one randomly and declare it the best, right? You’d try a few, see how your skin reacts, and then decide. That’s science in action.
Scientists observe the world, ask questions, test ideas, and then look at the evidence before drawing conclusions. It’s not about gut feelings or trends. It’s about facts and proof.4 Menopause research is built on decades of science. Understanding how to evaluate menopause research will help you rely on evidence-based menopause health advice rather than trends.
When it comes to health, not all studies are created equal. You’ve probably heard of clinical trials. These are considered the best, especially a specific type called a randomized controlled trial (RCT). In an RCT, scientists take a group of people, randomly assign some to receive treatment and others to a placebo (a “dummy” treatment), and then compare the results.5
Double-blind means neither the participants nor the scientists know who’s getting the real treatment and who’s getting the placebo. This helps avoid bias. If a menopause treatment passes one of these trials, it’s worth paying attention to.
Not all studies are created equal, and science has its own hierarchy of evidence.6 This hierarchy is essential when learning how to evaluate menopause research. Picture it as a pyramid.
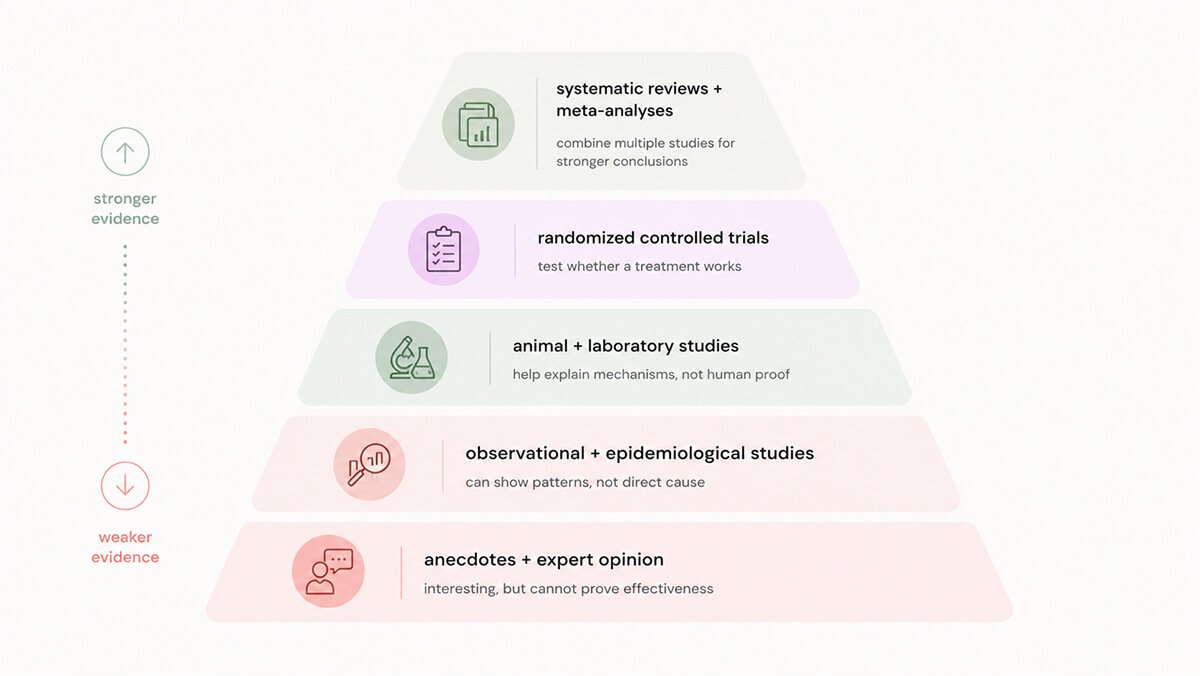
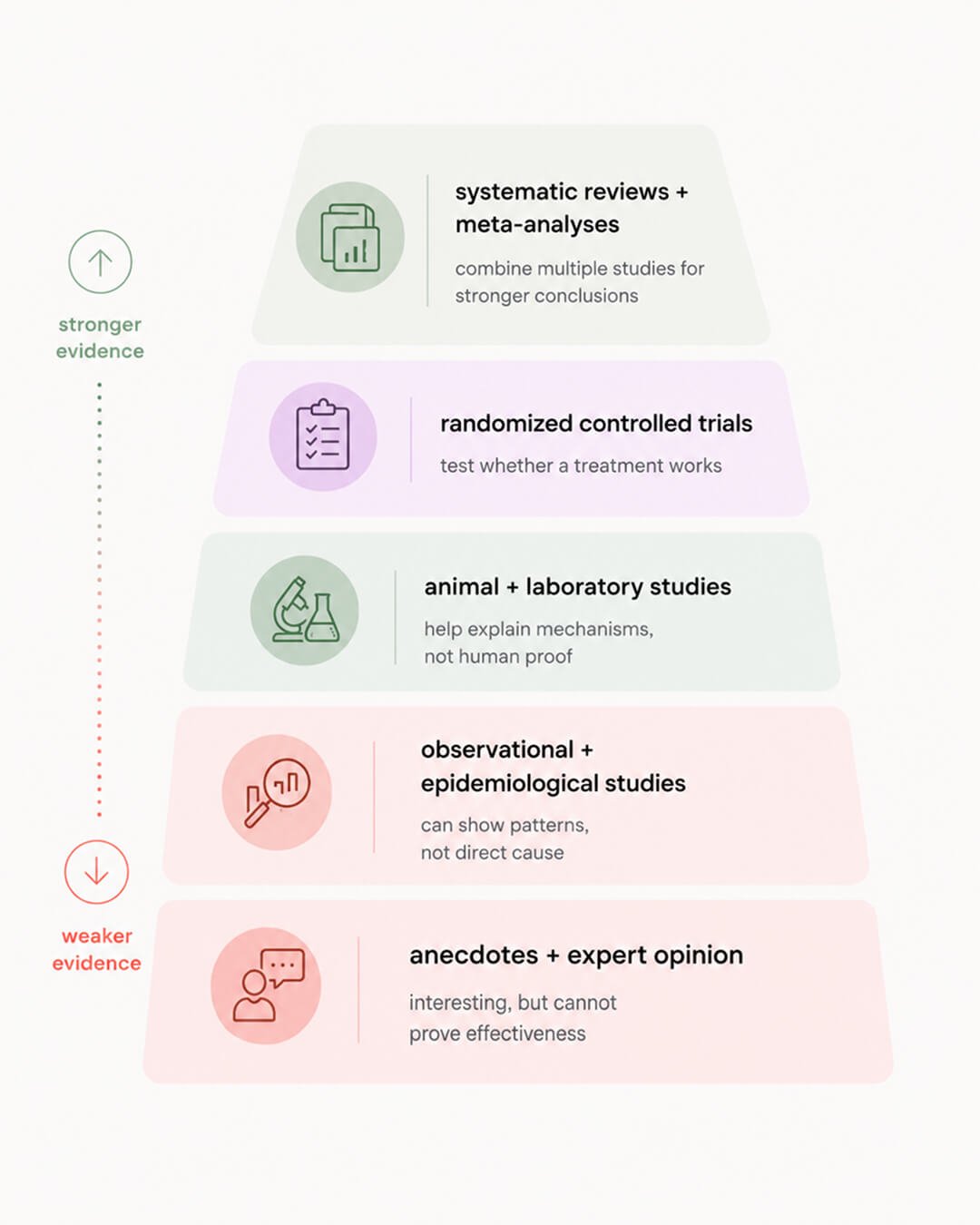
At the bottom, you have expert opinions and anecdotes, personal stories, or professional experiences. They can be interesting, but they don’t hold much weight when it comes to proving anything scientifically. Relying only on anecdotes contributes to menopause misinformation.
A bit higher up, we have observational studies. These are useful for spotting trends and correlations, but they can’t prove that one thing directly causes another. For example, observational research might show that women who exercise tend to feel better during menopause, but it doesn’t prove that exercise alone is responsible. Observational studies alone are not enough for evidence-based menopause health advice.
Epidemiological studies fall into the same level as observational studies. These studies look at large populations to identify risk factors and health outcomes. They help to establish broad patterns like the age of onset for menopause or associations between lifestyle factors and menopause symptoms. While valuable, these studies also don’t prove direct cause and effect. However, they can guide future research.
Animal studies come next. These involve testing treatments or hypotheses in animals to get a sense of how something might work in humans. Although animals aren’t a perfect match for humans, these studies are crucial for understanding biological mechanisms, particularly in early drug development and in working out how hormones act in different tissues.
Above that are randomized controlled trials (RCTs), the gold standard for scientific evidence. These studies carefully compare treatments to placebos, reducing bias and making their findings more trustworthy.
A separate bucket that draws data from different research would be systematic reviews and meta-analyses. These are like the superheroes of scientific research. A systematic review pulls together all the studies on a particular topic, evaluating their quality and summarizing the findings.7 A meta-analysis goes even further: it combines the data from multiple studies into one big analysis to get a clearer, more powerful result. This means that if a treatment has passed a meta-analysis, it’s not just good, it’s been tested and verified by pooling together a lot of high-quality evidence.8
You’ve probably seen posts on social media where someone claims that a particular herbal supplement completely “cured” their hot flashes overnight. This is a personal anecdote, and while it might sound compelling, it’s just one person’s experience. It doesn’t mean the supplement works for everyone, or even that it truly worked for them. Personal anecdotes are often used to create and spread menopause social media myths.
Compare that to a randomized controlled trial where scientists give one group of women the supplement and another group a placebo, tracking their symptoms over several months. If the supplement consistently reduces hot flashes in the group receiving it (and not just the placebo group), that’s a strong sign it’s effective. Better yet, if several RCTs are reviewed in a meta-analysis, the combined data gives an even stronger conclusion.
Social media is full of hearsay and anecdotes. Solid scientific evidence comes from well-designed studies that provide reliable menopause health advice, not one-off personal stories.
A few patterns repeat so often that once you spot them, you’ll see them everywhere. Recognizing these patterns helps you identify menopause misinformation quickly.
One small study doing heavy lifting. When “clinically proven” rests on a single trial, especially a small one, it rarely provides strong evidence for menopause health advice. Evening primrose oil is a good example. A 2025 meta-analysis of six trials found no statistically significant reduction in hot flash frequency or intensity versus placebo, with the evidence graded as moderate to low quality.9 Product pages keep implying otherwise.
Animal data dressed as human data. Mechanisms worked out in mice or cell culture are useful for generating hypotheses. They do not prove that a compound does anything meaningful in a menopausal woman at a dose she can actually take. “This molecule supports adrenal function in rats, therefore it helps you in perimenopause” is a rhetorical jump wearing a lab coat. This confusion is common in menopause social media myths.
Surrogate outcomes replacing real ones. The most expensive version of this is comprehensive hormone panels marketed as essential for perimenopause. Perimenopause is a clinical diagnosis based on age, cycle pattern, and symptoms. Follicle-stimulating hormone (FSH) fluctuates so dramatically across the transition that a single blood draw can be actively misleading.10 Major guidelines (NICE, the International Menopause Society, the European Menopause and Andropause Society) do not recommend routine hormone panels for women over 45 with typical symptoms.11
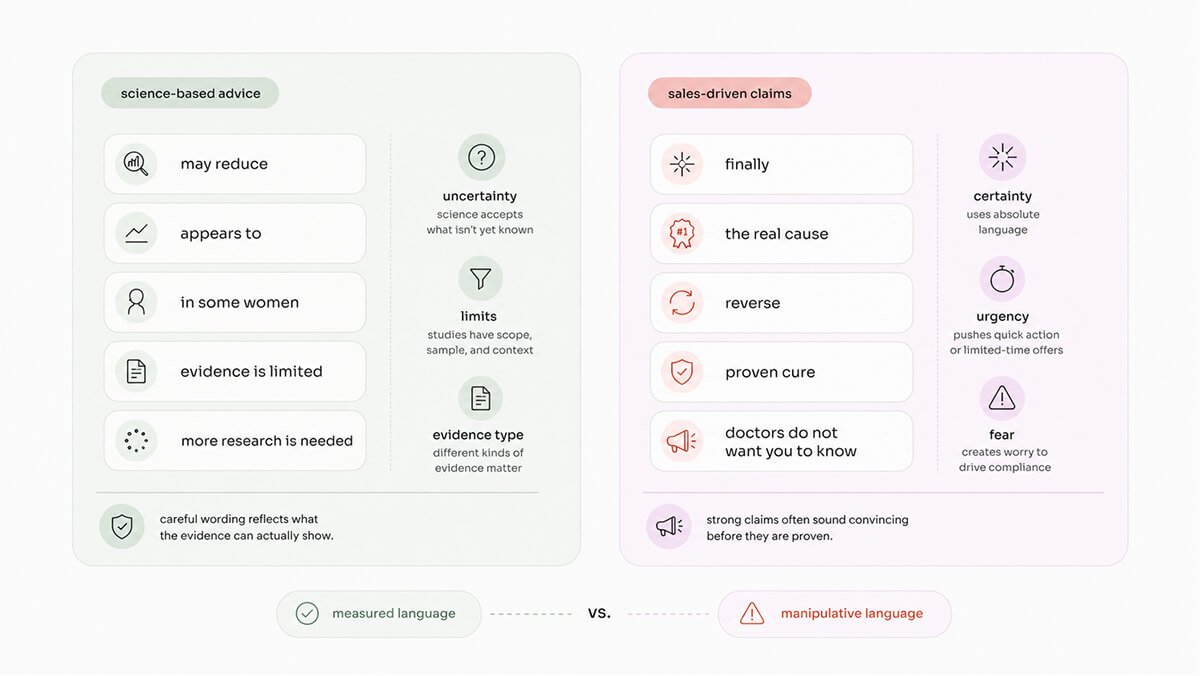
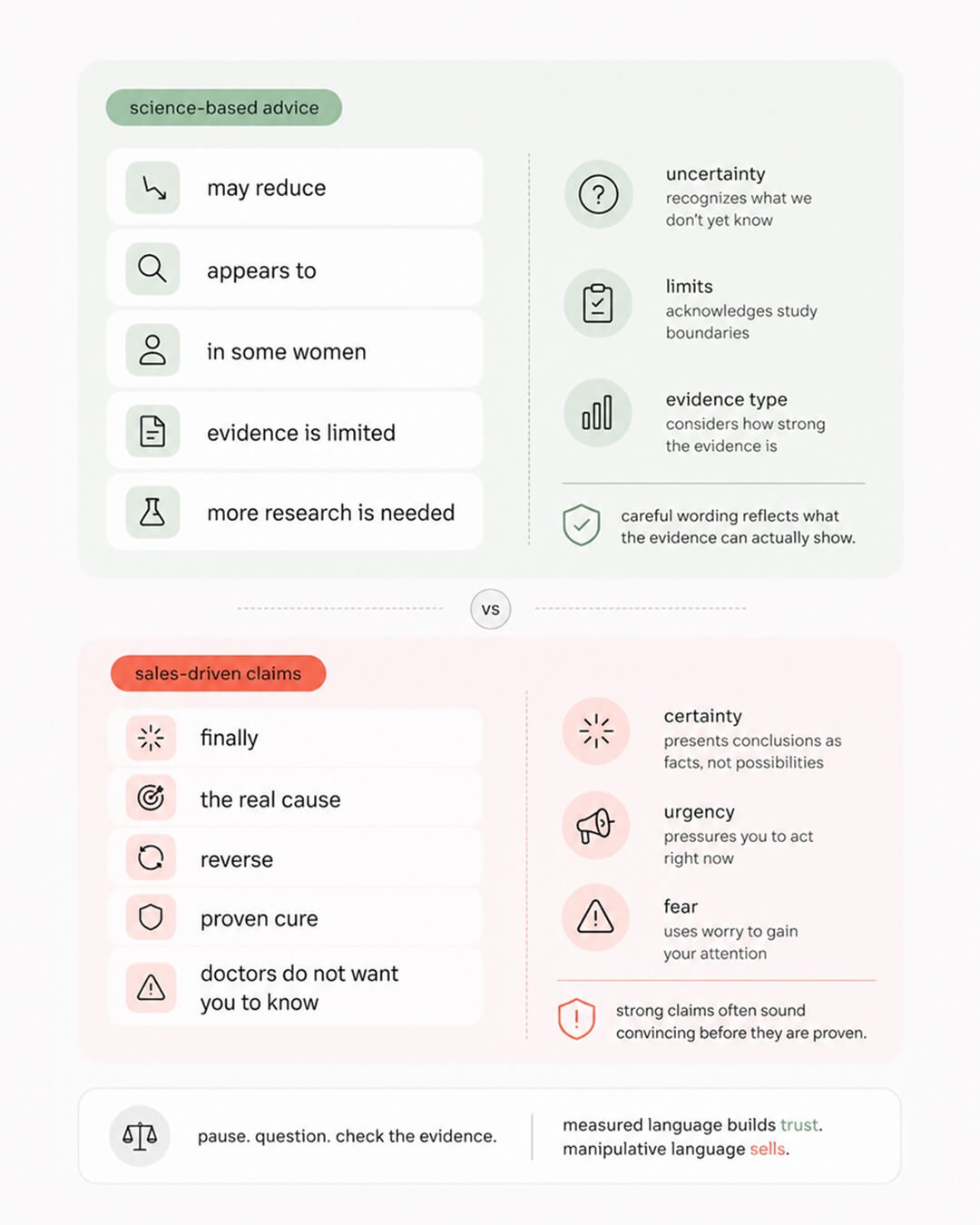
Absolute language. Evidence-based writing says may reduce, appears to, in some women, and names its limits. Sales language says finally, the real cause, reverse, doctors don’t want you to know. The first register is calibrated to what the data can hold. The second is calibrated to what a shopping cart can hold.
Understanding the pyramid gives you a solid foundation evaluating if menopause health advice is actually science-backed. But in real life, you don’t have time to read a meta-analysis between meetings. You need a fast filter.
Before acting on any menopause claim you see online, in a clinic, or in a WhatsApp group, run it through these five questions. Credible menopause advice usually survives all five. Weak menopause advice tends to fall apart by question two. This framework is one of the fastest ways to evaluate menopause research.
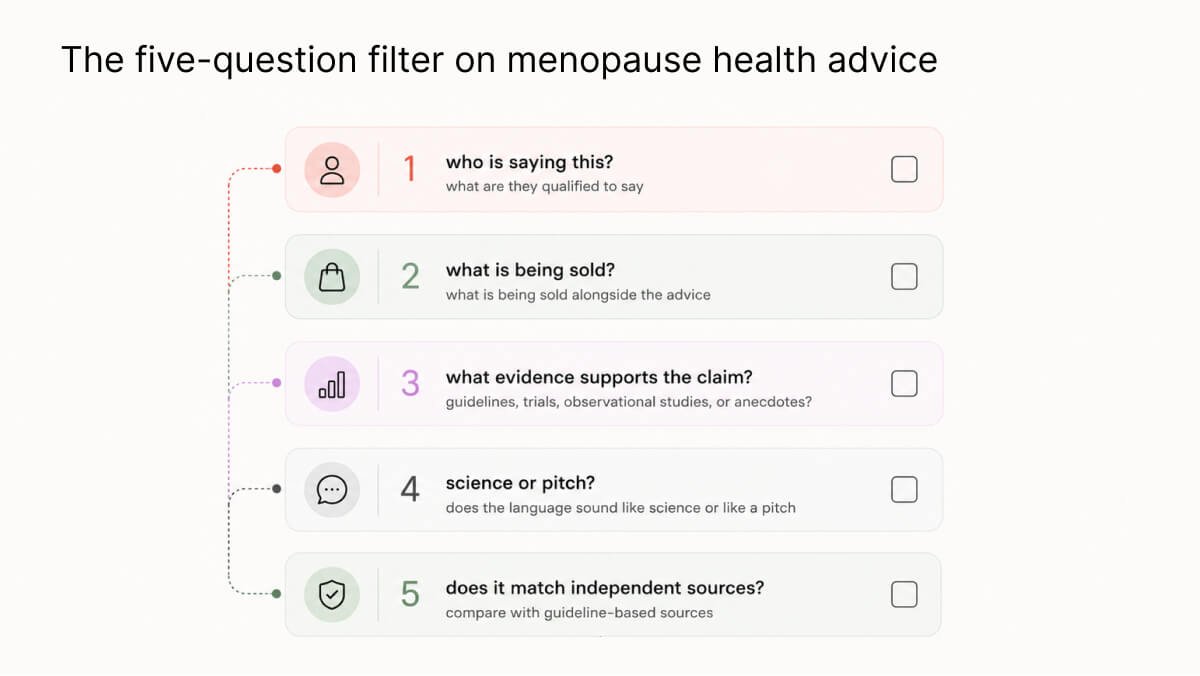
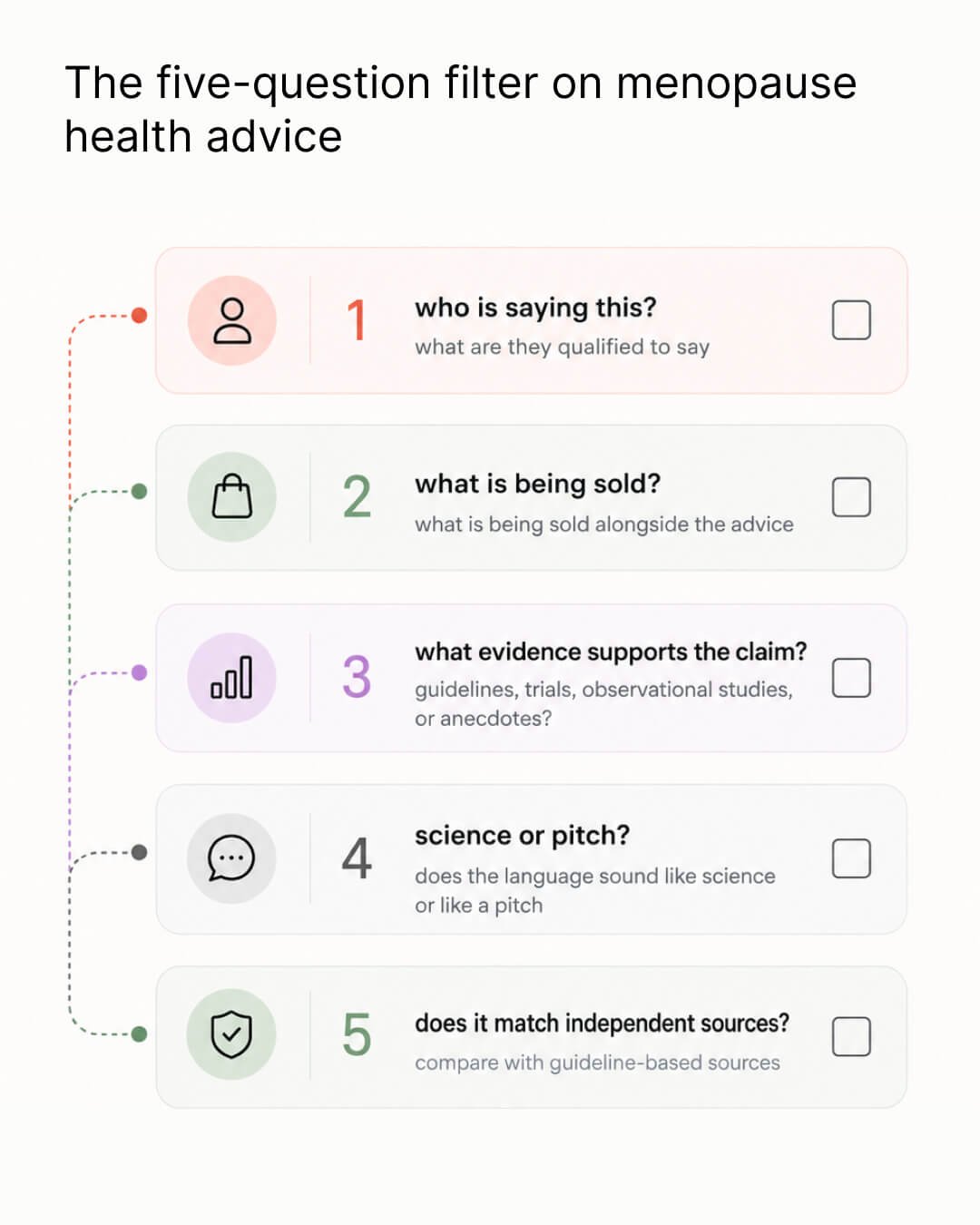
You already know how to do this. When a vendor walks into your office with a deck full of testimonials and zero data, you notice. When someone quotes a pilot study as if it were a phase III trial, you notice. When a founder insists the competitor is hiding the real numbers, you notice. The filter you use every week at work is the same filter that protects your body, your bank balance, and your cognitive edge.
Science helps you make decisions based on facts, not guesses or trends. Understanding the basics, like why randomized controlled trials and meta-analyses matter, empowers you to make more informed health decisions. And when you’re navigating perimenopause and postmenopause alongside a demanding career, you deserve the best, most reliable information.
So the next time you hear about a new study on menopause, ask yourself: What’s the evidence? Was it tested in a rigorous clinical trial? Is this based on a systematic review or meta-analysis? Who is saying it, and what are they selling? When you approach your health like a scientist, you’re in the driver’s seat.
Dr. Jūra Lašas
1.
Grand View Research. Menopause Market Size, Share & Trends Analysis Report. (2025) https://www.grandviewresearch.com/industry-analysis/menopause-market
2.
McCartney M, Morgan-Young R, Sullivan F, et al. Does online information about hormone replacement therapy (or menopause hormone therapy) reflect indications from the British National Formulary and guidance from the National Institute for Health and Care Excellence: a cross-sectional study of UK media. (2025) https://doi.org/10.1136/bmjopen-2024-094773
3.
Christakis M K, Roebotham T, Sterry S, Koshkina O. Menopause misinformation is harming care. (2025) https://doi.org/10.1136/bmj.r1695
4.
Harris, E. Science and Science Teaching. (1942) https://doi.org/10.1038/149734A0
5.
Hariton, E. et al. Randomised controlled trials – the gold standard for effectiveness research. (2018) https://doi.org/10.1111/1471-0528.15199
6.
Brighton, B. et al. Hierarchy of Evidence: From Case Reports to Randomized Controlled Trials. (2003) https://doi.org/10.1097/01.blo.0000079323.41006.12
7.
Siddaway, A. et al. How to Do a Systematic Review: A Best Practice Guide for Conducting and Reporting Narrative Reviews, Meta-Analyses, and Meta-Syntheses. (2019) https://doi.org/10.1146/annurev-psych-010418-102803
8.
Barker, F. et al. Synthesizing medical evidence: systematic reviews and metaanalyses. (2005) https://doi.org/10.3171/FOC.2005.19.4.6
9.
Larki, M. et al. The Effect of Evening Primrose Oil on Menopausal Symptoms Management: A Systematic Review and Meta-Analysis. (2025). https://doi.org/10.34172/jcs.025.33570
10.
Randolph, J. et al. Change in estradiol and follicle-stimulating hormone across the early menopausal transition. (2004). https://doi.org/10.1210/jc.2003-031183
11.
Panay, N. et al. International Menopause Society recommendations and key messages on women’s midlife health and menopause. (2025) https://doi.org/10.1080/13697137.2025.2585487

Healthy Body & Mind
Brain & Mind Wellness

Treatments & Supplements

Understanding Menopause

Scientific Research

Understanding Menopause

Lifestyle & Self-Care

Scientific Research

Eat to Thrive

Scientific Research

Treatments & Supplements

Understanding Menopause

Understanding Menopause
Understanding Menopause

Lifestyle & Self-Care
We use cookies and similar technologies to ensure the proper functioning of our website, personalize content, provide social media features, and analyze traffic. By clicking “I Agree”, you consent to the use of these technologies.
No results




