16 December 2025
Perimenopause Symptoms at Work: An Evidence-Based Guide for Professional Women

Reading time 15 min

Reading time 15 min
Perimenopause symptoms at work can begin subtly. You read the same email three times because you can’t understand it. The word “budget” disappeared mid-sentence in your last meeting and you covered it with “money plan” before anyone noticed. Perimenopause symptoms at work are real, they show up where the cognitive load is heaviest, and most workplaces still treat them as a personal weakness. The latest systematic review on menopause symptoms at work tells a different story, and that story changes what you should actually do.
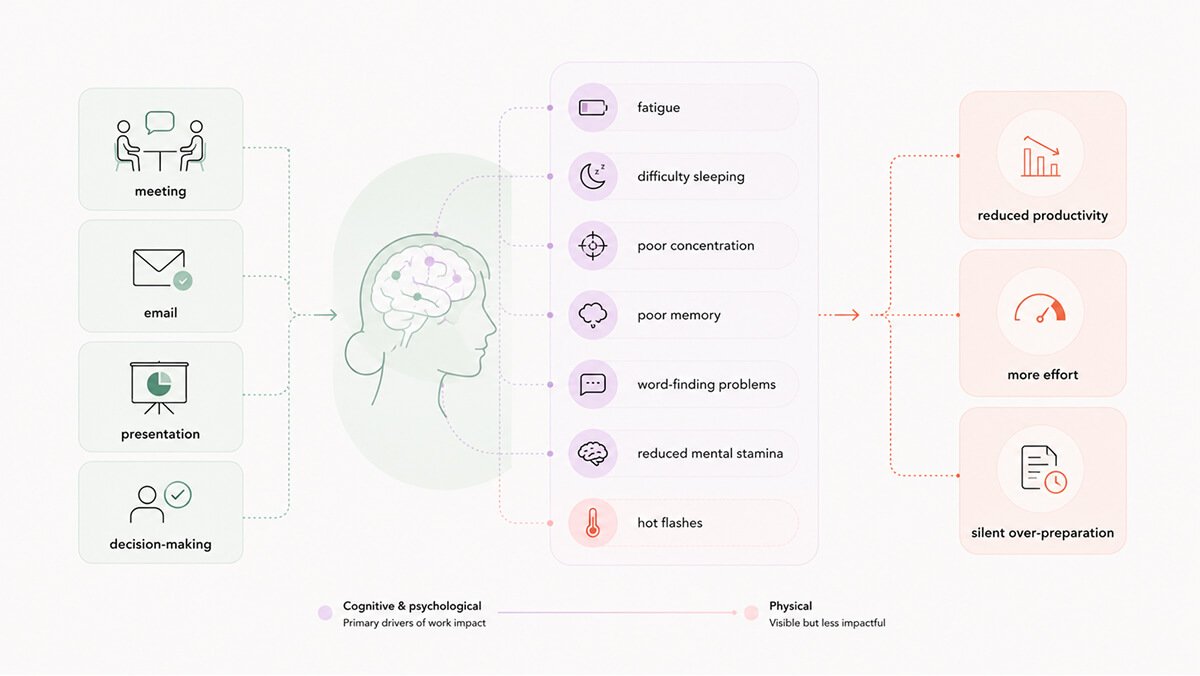
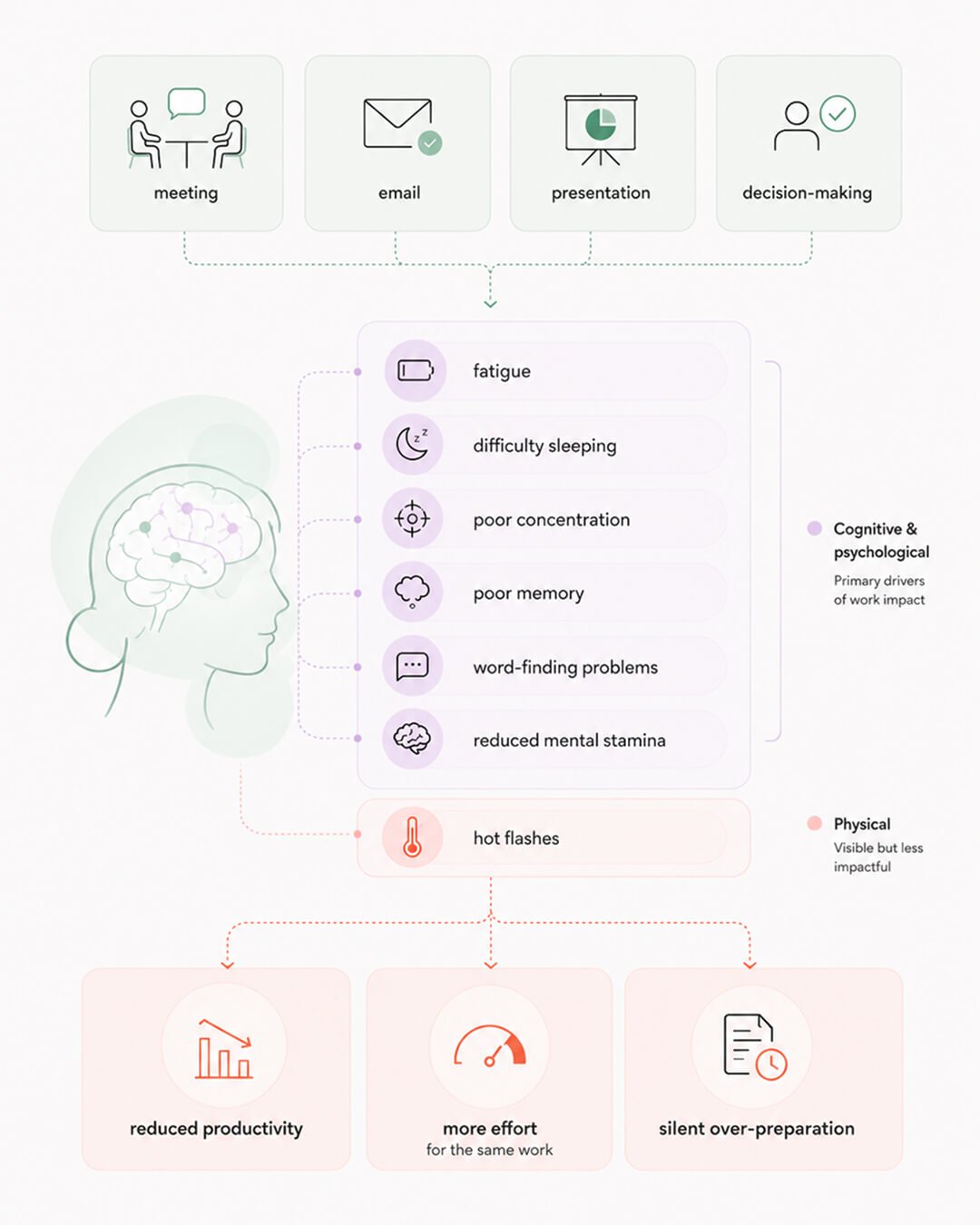
When most people picture menopause symptoms at work, they picture a hot flash. That is not what the data shows.
Among 407 women in an Irish hospital, the menopause symptoms most affecting them while at work were fatigue (54%), difficulty sleeping (47%), poor concentration (44%), and poor memory (40%). 65% reported reduced work performance and 18% had taken sick leave. The symptoms with the strongest links to issues at work were the psychological and neurocognitive ones, not the vasomotor ones.1
Translate that into your day. You read the same paragraph three times and it doesn’t sink in. You walk into a meeting knowing what you want to say and the word for it is gone. You sit in a strategy session you used to dominate and feel a half-step behind. You go home with nothing left.
The fatigue piece deserves a closer look because it is the symptom most often dismissed as a general midlife condition. Among working women 40+, fatigue is one of the strongest independent predictors of lower work productivity, and it is heavily driven by worse sleep quality rather than total sleep hours.2 Night sweats wake you briefly without you remembering, and the broken-up sleep leaves you with the same eight hours in bed and a fraction of the cognitive recovery. A bad night affects the next day’s performance.
Curious Fact. In a 2025 study of Irish women, only the psychological symptoms (mood, anxiety, irritability) predicted lower work ability. The physical (joint pain, hot flashes) and urogenital symptoms did not.³ The symptoms most workplace policies target are not the ones actually linked to whether you can do your job.
Organizational policy still focuses on the physical menopause symptoms at work. Cooling vests, fans, breathable uniforms, temperature-controlled meeting rooms. They help with what they target, but they do not address the symptoms most affecting work performance.
A separate finding deepens the picture. Among 476 perimenopausal and postmenopausal women in a higher education sector, high supervisor support, full-time employment, and control over workplace temperature were each independently associated with lower menopausal symptom reporting.4 The workplace does not only shape how symptoms affect work. It appears to shape how severe symptoms feel in the first place.
The economic toll is large. The Mayo Clinic study of 4,440 employed women aged 45 to 60 estimated $1.8 billion in lost productivity in the United States annually from missed workdays alone. The figure doesn’t even account for cut hours, declined promotions, or early exits.5 The European Menopause and Andropause Society has flagged menopause in the workplace as a workforce retention issue requiring policy change.6
Historically, menopause symptoms at work were treated as a personal productivity problem to manage. Women powered through, took care of the symptoms, and were told to fix themselves.
Across the 10 highest-quality studies on menopause and work in the most recent systematic review, menopause symptoms at work were not consistently associated with worse work outcomes.⁷ Menopause symptom severity may impact work outcomes, but findings were mixed. Employment conditions, socioeconomic factors, and personal circumstances consistently predicted work ability.
Being in perimenopause or posmenopause does not, on its own, predict that your career will suffer. What predicts worse work outcomes is the combination of severe symptoms and a workplace that has not been designed to absorb them.
The Mayo Clinic data showed that women with the most severe menopause symptoms were 15.6 times more likely to report troubles (missed days, cut hours, declined promotions, early exits) than women with mild symptoms.5 Severe menopause symptoms collided with workplaces that were not built to accommodate them.
This pattern is also evident in long-term studies of working women in the UK. Struggles in the workplace were closely linked to financial stress, lower self-reported health, depression, and poor social conditions on the job. Interestingly, the physical nature of the work wasn’t a primary factor. Across different nations, the conclusion remains the same: while symptoms are genuinely difficult, a woman’s overall environment ultimately dictates whether she can manage her workday or if it becomes overwhelming.8
Research among Irish employees shows that strong organizational support can actually reduce the intensity of symptoms. Similarly, a study of nearly 600 Japanese women found that while more symptoms typically lowered job performance, this was heavily influenced by health habits, existing illnesses, and family responsibilities. Ultimately, a clear picture emerges: while the severity of the experience is important, both the workplace environment and a person’s private life determine how much it truly impacts their career.9
The fundamental question is whether your workplace was designed to accommodate your biological reality. For most women in leadership, the reality is that it wasn’t. This structural mismatch is a genuine flaw in workplace design, and it is a systemic issue rather than a personal failure.
The cognitive functions most affected during perimenopause are
Those are the same functions senior leadership runs on every day.
A small change in retrieval speed is not visible in routine work and can be visible in a board presentation, a tense negotiation, or a high-stakes hire. The Irish hospital data showed psychological and neurocognitive symptoms had the strongest links to reduced performance and career decisions.1 Severity makes that link sharper. A Dutch study comparing healthy employees to those seeking menopause treatment found that women experiencing symptoms were over eight times more likely to struggle with their work capacity. Additionally, more than 75% of these women reported significant challenges in meeting the physical and mental requirements of their roles.10
High visibility can be a double-edged sword. As you rise in seniority, your performance is more closely watched, leaving less room for minor mistakes before others begin to question your professional competence. Women in leadership or male-dominated fields are often the most hesitant to speak up, having spent years proving they belong.11 These risks are supported by data: a 2024 study of US working women found that over half feared being seen as less capable due to menopause, while 77% faced actual work challenges.¹² The most striking discovery, however, was the massive disconnect between corporate support and employee needs; while nearly 70% of women wanted formal policies and trained managers, such resources were available in only a tiny fraction of workplaces.
To manage, you adapt. You rely on notes for things you once memorized, over-prepare for meetings, tackle complex tasks during your peak morning hours, and pause before answering difficult questions. While these are smart adjustments, this silent compensation carries a long-term cost. Women who use flexible schedules to manage symptoms without broader support often fall into a cycle: they overwork when feeling well but decline high-profile projects or skip key networking events when struggling.13
While this keeps performance steady in the short term, it quietly stalls career growth. This decline remains unnoticed by the organization until the damage is done. Ultimately, personal coping and workplace structure are both essential. If an employer accommodates your biological needs, those needs cease to be a professional barrier. If the workplace fails to adapt, you end up paying for that lack of support with your own career advancement.
Much of the workplace advice found online lacks rigorous testing. However, a few specific interventions have been proven effective in clinical trials that directly measure work performance. Distinguishing between general tips and proven strategies is vital when advocating for your needs.
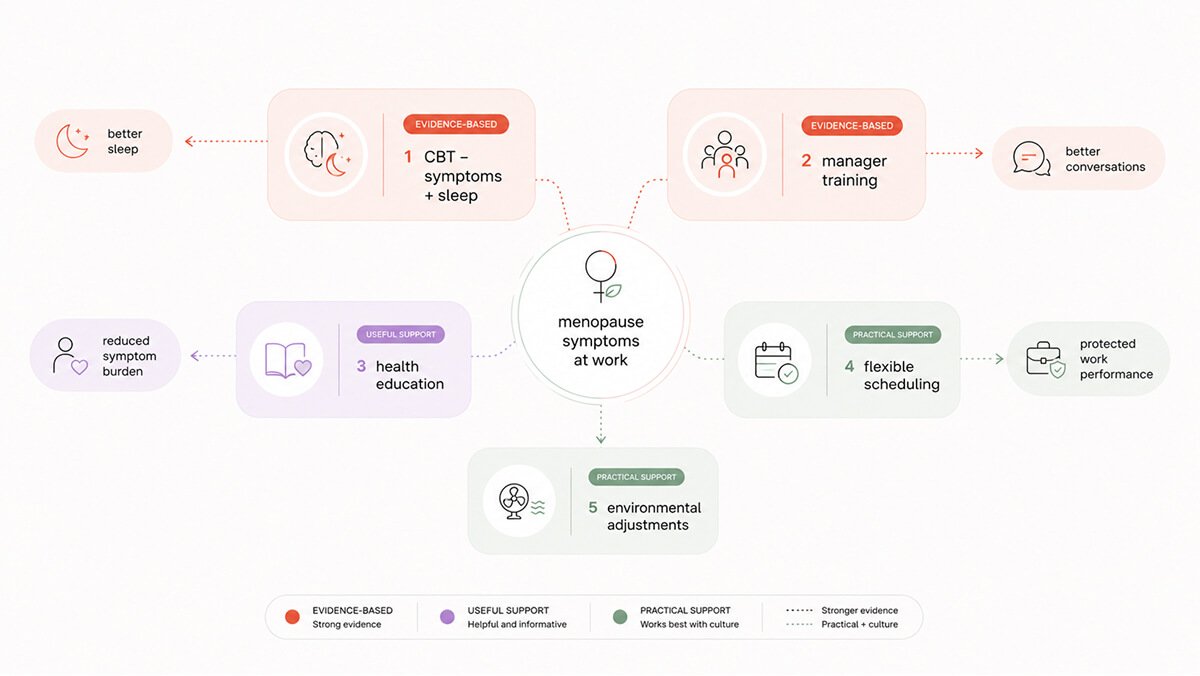
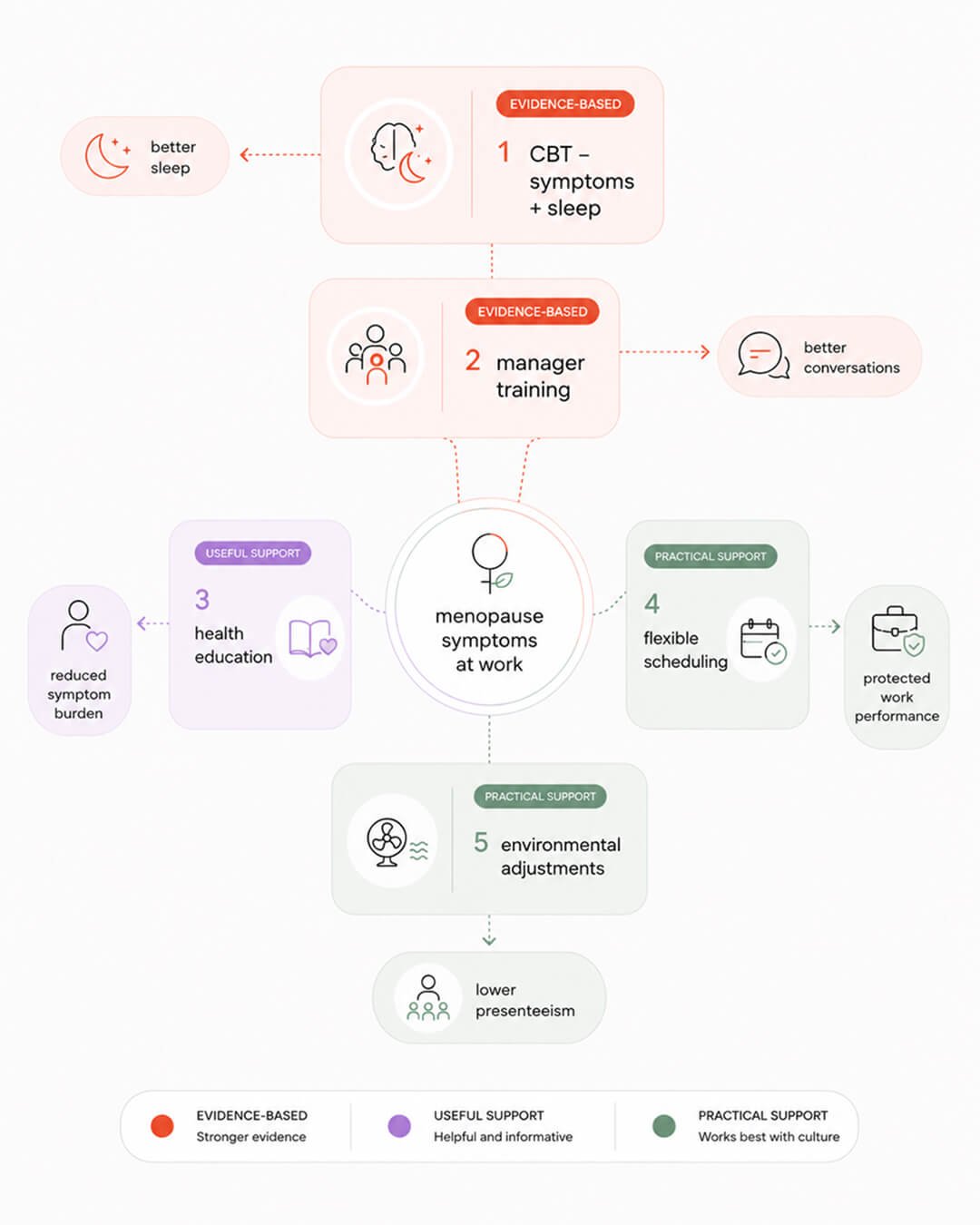
Cognitive Behavioral Therapy (CBT) for menopause currently has the strongest evidence for workplace success. One study involving 124 working women showed that a self-guided CBT program significantly reduced the impact of hot flashes, improved sleep, and decreased “presenteeism” – being physically present but mentally unproductive. These improvements lasted for months. Similar benefits have been found for CBT focused on insomnia, which enhances daytime productivity and overall quality of life.14,15
The effectiveness of CBT lies in its ability to break the “catastrophizing loop” that makes symptoms worse. For instance, if you feel a hot flash during a presentation, the fear of it can trigger a stress response that intensifies the physical heat. Similarly, panicking over a forgotten word uses up the mental energy needed to finish your thought. CBT teaches you to reframe these symptoms in the moment, stopping the cycle of anxiety. Because these protocols are brief, structured, and available digitally, you can implement them yourself without engaging your employer.
Manager training is another highly effective strategy supported by evidence. Short, 30-minute online sessions have been shown to significantly improve a manager’s knowledge and confidence when discussing menopause with their team. In fact, over 90% of managers who completed these programs found them helpful. Educational initiatives for employees are equally beneficial, as they improve confidence and reduce lost productivity. Both methods are valuable because they spare you from having to educate your supervisor while managing your own symptoms.16,17
The most successful programs focus on three key areas: understanding how menopause manifests in a professional setting, learning how to offer support without overstepping boundaries, and identifying practical, reasonable workplace adjustments. Implementing these changes is straightforward and does not require a medical background.
Providing health education for women is a strategy supported by moderate evidence. Understanding the biological changes taking place naturally reduces anxiety and helps women make more informed choices regarding sleep, exercise, and medical treatment. This knowledge changes how a woman perceives her own symptoms, making them feel more manageable. While education by itself won’t solve every challenge, it lessens the overall impact of symptoms while other, more intensive interventions take effect.17
Flexibility is the most sought-after workplace adjustment, though it comes with specific conditions. Women consistently prioritize flexible hours, remote work, and the option for short breaks as their most valued support.1 However, when flexibility is offered without an informed manager or an open company culture, it often leads to the “invisible career drag” where professional growth stalls. For flexibility to be effective, it must be integrated into a genuine support system. Without that foundation, it merely masks the impact of symptoms rather than improving the workplace environment that creates the challenges in the first place.13
Environmental adjustments have strong biological logic but lack extensive testing in controlled trials. Features like temperature control, improved ventilation, breathable uniforms, access to cold water, rest areas, and seating near exits or windows are recommended by nearly every expert guideline, even though they are rarely studied rigorously. Despite the lack of formal data, the biological benefits are clear and the cost of implementation is low.6
The best data supports psychological tools and changes in organizational culture as the most effective solutions. In contrast, physical accommodations, like temperature and environmental controls, have less direct evidence but are inexpensive and biologically logical. These two approaches are most effective when used together. Having temperature control without manager training simply results in women managing their symptoms alone in a cooler office. Conversely, having trained managers in an unadjustable environment leads to supportive conversations in a workplace that remains physically uncomfortable.
Most of us are not waiting for a formal company policy to manage our daily workload. There are six evidence-based strategies you can implement immediately to help navigate this transition.
Prioritize sleep as a foundation. Interrupted sleep worsens every cognitive symptom of perimenopause and is a leading cause of lower productivity. Cognitive Behavioral Therapy for Insomnia (CBT-I) is clinically proven to help and is available through self-guided digital tools. Improving your sleep usually offers the highest mental return on investment.2,15
Align your schedule with your brain energy. Cognitive symptoms in perimenopause fluctuate. Some mornings you are sharp and some afternoons you are not. Block out your most mentally taxing work, like strategy or complex writing, for the hours when you feel sharpest. Save routine emails and administrative tasks for your lower-energy periods. Since multitasking and switching between tasks are harder on your working memory now, try to focus on one thing at a time.
Create an “external brain.” Use checklists, digital alerts, and dedicated apps to capture action items in real time. Occupational health experts recommend such tools to best manage perimenopause and menopause symptoms at work that affect your working memory.6 By documenting your tasks externally, you free up mental energy for the high-level decisions that actually require your focus.
Proactively control your environment. Use breathable layers, keep cold water nearby, and use a desk fan or sit near windows during meetings. You can request these adjustments using professional, performance-based language, such as “I’m more productive when it’s cooler” without needing to disclose medical details.
Identify patterns through tracking. Instead of relying on your memory, keep a simple log of your sleep quality, workload, and symptom spikes. Seeing these connections on paper or a screen provides objective data that is invaluable for both medical consultations and professional discussions about your needs.
Seek medical advice early. Hormone therapy and other treatments are highly effective for managing hot flashes and sleep issues, which in turn often clears “brain fog.” Consulting with a healthcare provider ensures you don’t simply accept exhaustion and memory lapses as a new normal.
Perimenopause symptoms are a documented reality in the professional world. The data indicates these challenges only become career-threatening when severe symptoms meet a workplace that lacks the infrastructure to handle them. The most effective solutions focus on workplace culture and psychological framing as much as biology. While the transition is difficult, the tools exist to manage it, even while the systems around you are still catching up.
The cognitive changes many women notice at work are not imagined. They reflect measurable, temporary changes in brain systems involved in memory, focus, and executive function.
Brain imaging studies show that during perimenopause the brain goes through a period of reorganization.
Gray matter volume can temporarily decrease in the hippocampus, a region central to memory. Metabolic activity shifts in the prefrontal cortex, which supports planning, decision-making, and cognitive control. At the same time, patterns of neural connectivity change as the brain adapts to fluctuating hormone levels.
This is not cognitive decline. It is a transitional phase in how the brain functions under hormonal change.
Dr. Jūra Lašas


Research shows 65-80% of women experience menopause symptoms, and 25-40% report these symptoms make work genuinely more difficult. Cognitive symptoms (brain fog, memory issues, poor concentration) affect work performance most, particularly in roles requiring sustained focus and decision-making.
In the USA, menopause symptoms may qualify for ADA accommodations if they substantially limit major life activities. Reasonable accommodations might include flexible schedules, temperature control, quiet workspace, or reduced meeting density. Documentation from a healthcare provider helps.
There is no single right answer. This decision depends on your workplace culture, your relationship with your manager, and whether any adjustments would genuinely make a difference to how you function at work. Some women find that being open leads to practical support. Others choose to manage symptoms privately, and that can be just as valid. Regardless of what you decide, keeping a record of symptoms is useful. It supports medical care and gives you context if workplace conversations become necessary later on.
The strongest evidence supports manager training and brief cognitive behavioral therapy, particularly for symptom coping and work functioning. Flexible work arrangements can reduce symptom burden by allowing women to align demanding tasks with higher-energy periods. Environmental adjustments such as temperature control and access to quiet rest areas can meaningfully reduce discomfort during the workday. Health education also plays a role by improving symptom recognition and self-management. The best outcomes are seen when workplace strategies are combined with appropriate medical care rather than used in isolation.
For most women, cognitive symptoms are most noticeable during late perimenopause and the early postmenopausal years, roughly the two to five years surrounding the final menstrual period. This is when hormonal fluctuations are greatest and the brain is adapting in real time. For many, symptoms ease after menopause as the brain adjusts to a new hormonal baseline. That said, experiences vary widely. Severity, duration, job demands, sleep, stress, and access to treatment all influence how long symptoms affect work functioning.
1.
Safwan, N. et al. Menopause in the workplace: Challenges, impact, and next steps. (2024) https://doi.org/10.1016/j.maturitas.2024.107983
2.
Whiteley, J. et al. The Impact of Menopausal Symptoms on Quality of Life, Productivity, and Economic Outcomes. (2013) https://doi.org/10.1089/jwh.2012.3719
3.
O’Neill, M. et al. Impact of menopausal symptoms on work and careers: a cross-sectional study. (2023) https://doi.org/10.1093/occmed/kqad078
4.
Faubion, S. et al. Impact of Menopause Symptoms on Women in the Workplace. (2023) https://doi.org/10.1016/j.mayocp.2023.02.025
5.
Faubion, S. et al. Menopause and the workplace: consensus recommendations from The Menopause Society. (2024) https://doi.org/10.1097/GME.0000000000002415
6.
Jack, G. et al. Menopause in the workplace: What employers should be doing. (2016) https://doi.org/10.1016/j.maturitas.2015.12.006
7.
D’Angelo, S. et al. Impact of Menopausal Symptoms on Work: Findings from Women in the Health and Employment after Fifty (HEAF) Study. (2022) https://doi.org/10.3390/ijerph20010295
8.
Hardy, C. et al. Self-help cognitive behavior therapy for working women with problematic hot flushes and night sweats (MENOS@Work): a multicenter randomized controlled trial. (2018) https://doi.org/10.1097/gme.0000000000001048
9.
Potočnik, K. et al. Managing menopause transition in the workplace: The double-edged sword of flexible work. (2025) https://doi.org/10.1111/joop.70032

Mood & Energy Solutions

Fatigue Causes & Types
Fatigue Causes & Types

Workplace Strategies

Menopause at Work

Brain Fog at Work

Brain Fog at Work

Is This Perimenopause?

Is This Perimenopause?

Nutrition & Supplements
Workplace Strategies

Menopause Science

Menopause Science

Brain Fog Solutions
We use cookies and similar technologies to ensure the proper functioning of our website, personalize content, provide social media features, and analyze traffic. By clicking “I Agree”, you consent to the use of these technologies.
No results





