22 June 2026
Am I in perimenopause? Signs, symptoms & the science

Reading time 9 min.

Reading time 9 min.
Perimenopause typically begins in the mid-to-late 40s and is marked by changes in menstrual cycle length, brain fog, disrupted sleep, new-onset anxiety, and vasomotor symptoms such as hot flashes. Perimenopause diagnosis is based on age and symptoms, not a single blood test.
The question “Am I in perimenopause?” rarely comes up in a doctor’s office. It comes up mid-sentence, when you reach for a word and find nothing. At 3am, heart pounding for no obvious reason. On a Tuesday morning when you feel anxious and can’t explain why. Your periods are still quite regular, so you write all of it off as stress.
Brain symptoms are often the first signs of perimenopause, and they arrive years before periods become irregular. Let’s discover what’s actually happening: the symptoms, the biology, and how to figure out whether perimenopause is the thread connecting things you’ve been trying to explain separately.
Your ovaries are not responsible for how you’ve been feeling – it’s your brain.
It’s true, your ovaries produce estrogen and progesterone. But the brain has been running the entire show for decades. The hypothalamus and pituitary gland coordinate your reproductive cycle by sending monthly signals to the ovaries, reading the hormonal response, and adjusting accordingly. When the ovaries start losing follicles (eggs) in perimenopause, that feedback loop doesn’t wind down gently. The brain tries to compensate and generates the majority of what we call perimenopause symptoms.1
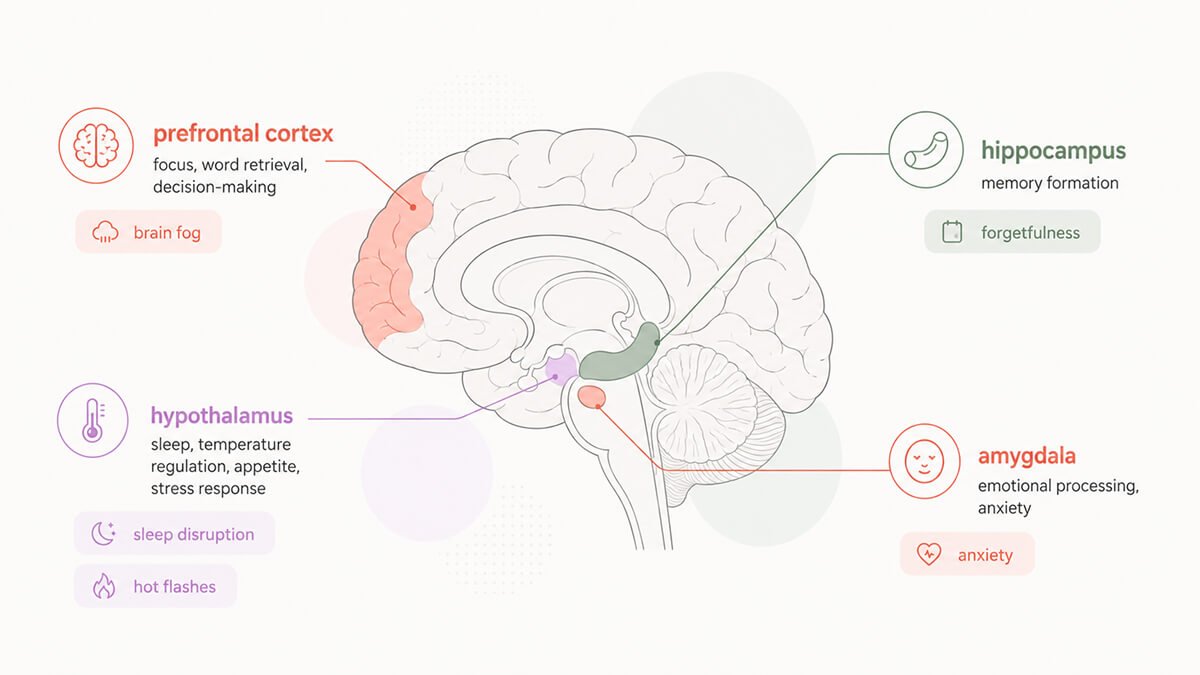
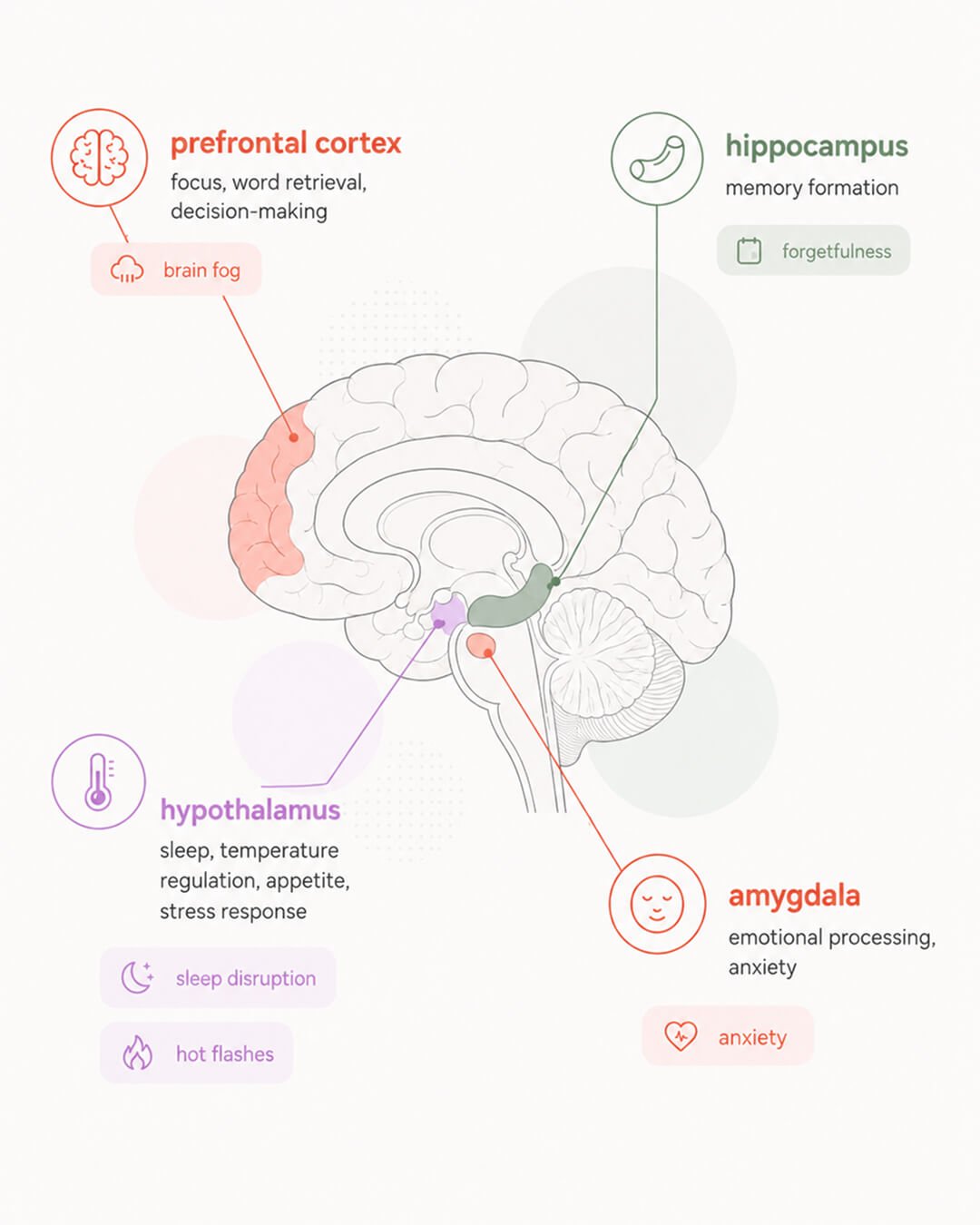
Estrogen has receptors throughout the brain: in the prefrontal cortex (focus, verbal retrieval, decision-making), the hippocampus (memory formation), the hypothalamus (temperature, sleep, appetite, stress response), the amygdala (emotional processing), and the brainstem. When estrogen fluctuates erratically, every one of those systems registers that change.
This is often the stage where women start asking, “Am I in perimenopause?” without realizing the answer may already be yes.
Up to 80% of perimenopausal and postmenopausal women report neurological symptoms – cognitive changes, mood swings, sleep disruption.2,4 Most are attributing it to stress or overwork. The biology points somewhere more specific.
The System Behind the Perimenopause Symptoms
Before getting into what you feel, it helps to understand the hormonal mechanism, because once you see it, the symptoms stop seeming random.
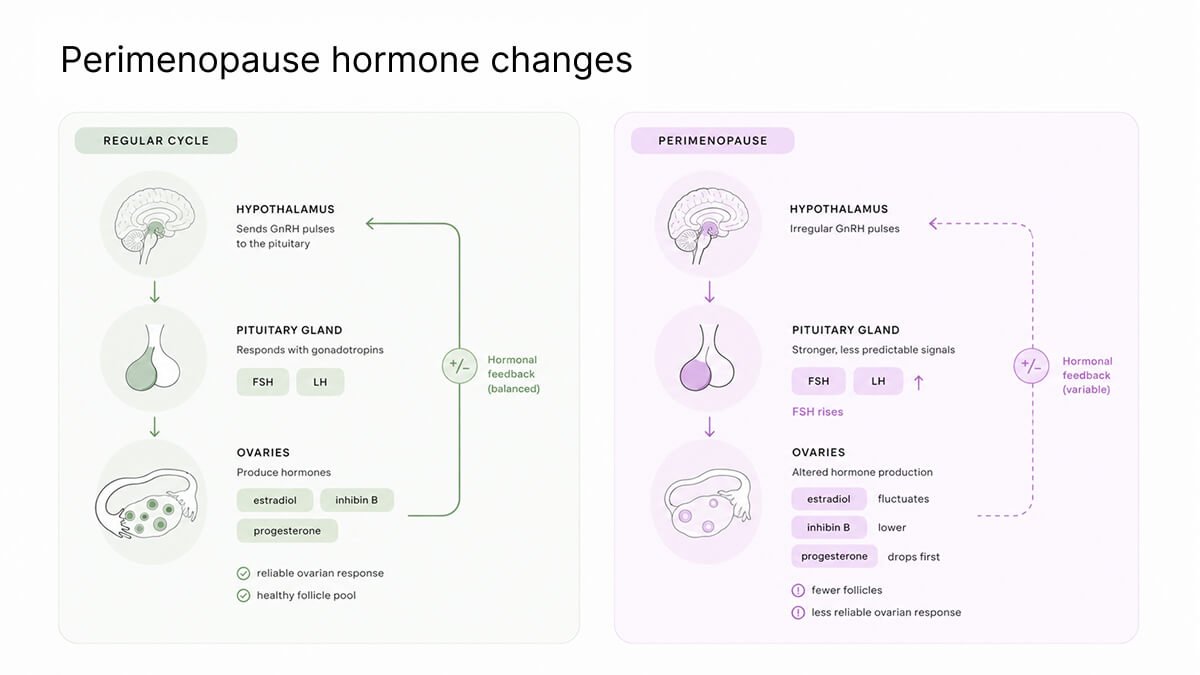
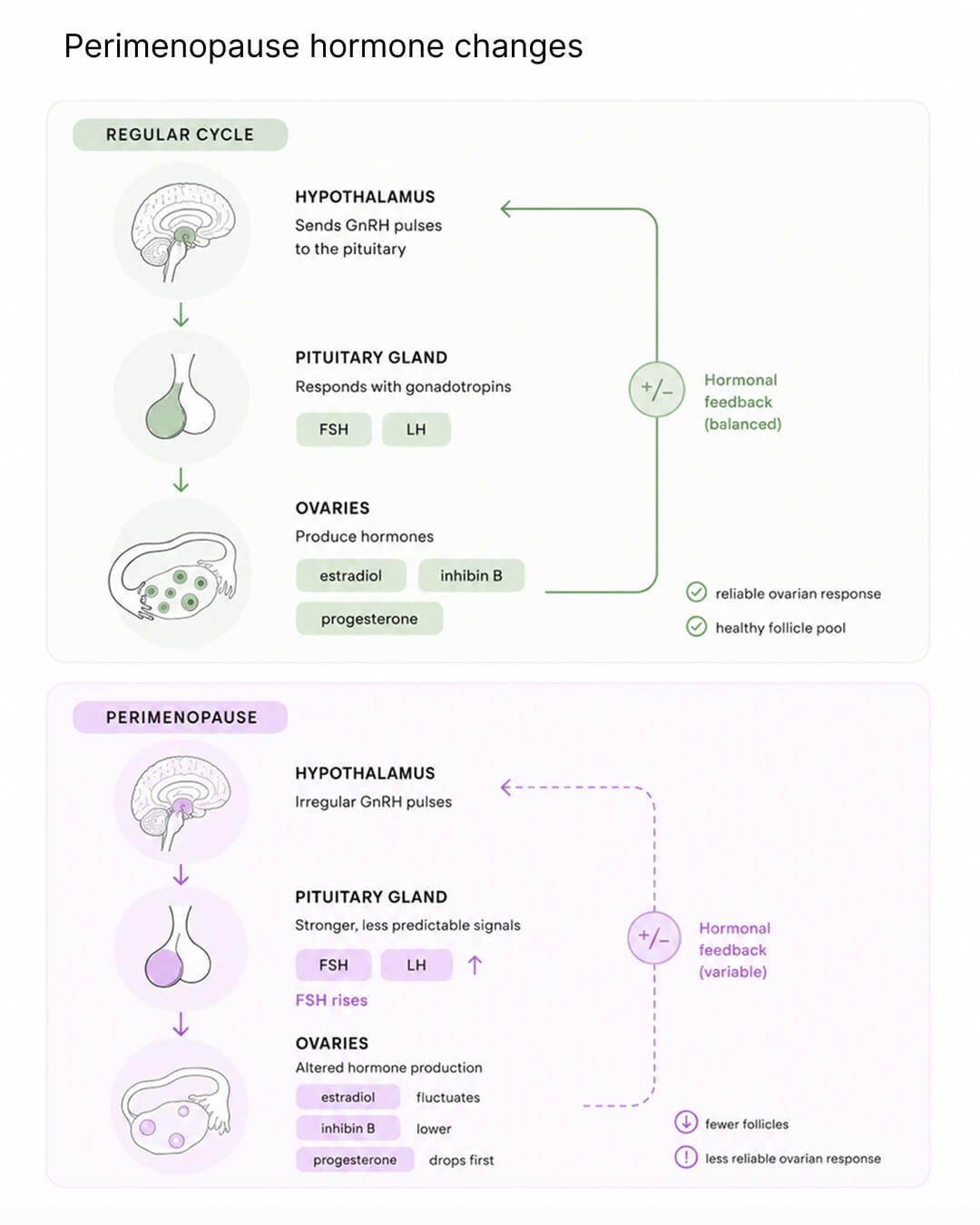
The HPO (hypothalamic-pituitary-ovarian) axis is the feedback system that has governed your hormonal cycle since puberty. The hypothalamus signals the pituitary; the pituitary signals the ovaries; the ovaries produce estradiol (a type of estrogen), inhibin B and progesterone; those hormone levels feed back to the brain, which adjusts the next cycle. It worked like clockwork for roughly 30 years.
In perimenopause, the ovaries begin losing follicles (eggs) and the system becomes unreliable. Progesterone drops first, as ovulation (release of eggs) becomes inconsistent.7 Estrogen doesn’t simply fall. In early perimenopause it fluctuates dramatically, often spiking above premenopausal levels before eventually declining. This is why symptoms feel so inconsistent from week to week. Also the reason why a hormone test on a single day is nearly meaningless for diagnosis.
The pituitary responds by producing more follicle-stimulating hormone (FSH), shouting louder at ovaries that are less and less able to respond. When this HPO axis goes, everything downstream goes with it: brain, heart, bones, gut, skin, bladder. Which is why perimenopause doesn’t feel like one thing.
Understanding this system helps answer the question: am I in perimenopause, or is something else going on?
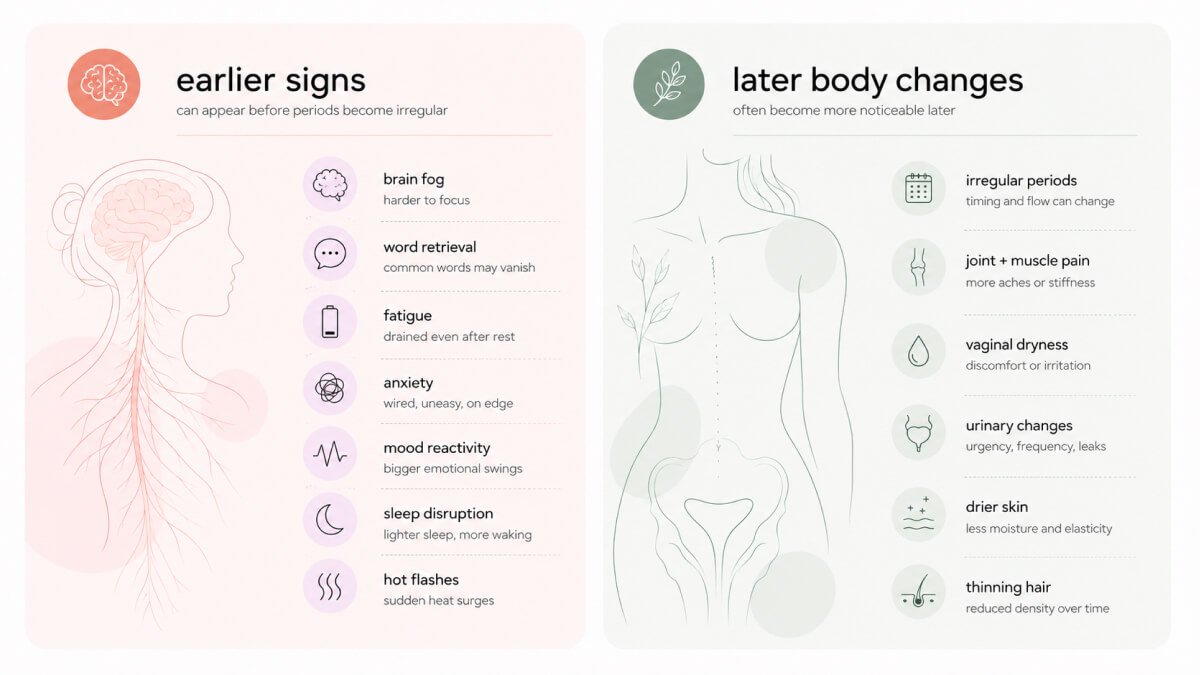
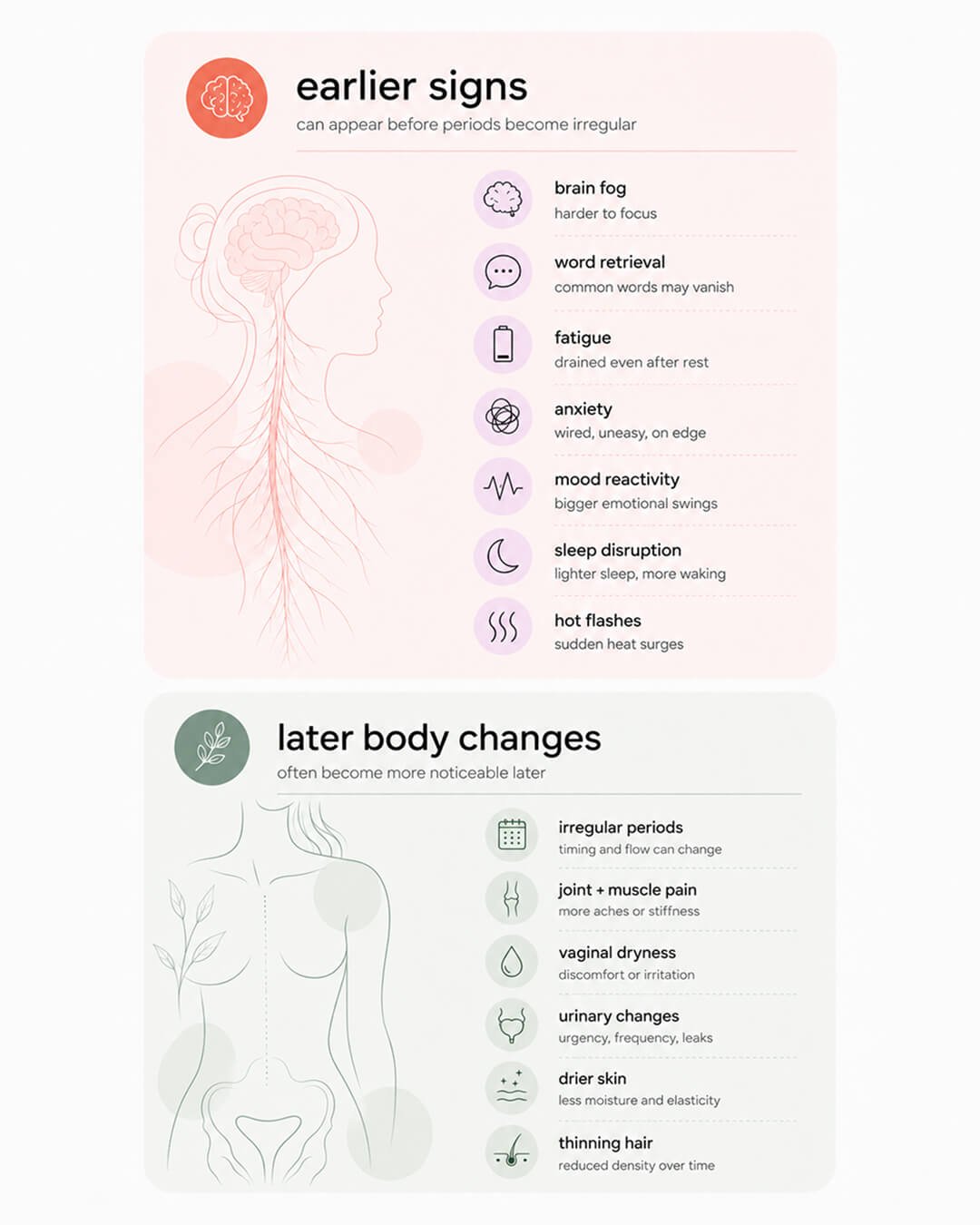
For many women asking “Am I in perimenopause?”, brain fog is the first clue. Brain symptoms are typically the first signs of perimenopause – before periods become irregular, before hot flashes, often years before most women would connect the dots to hormones. They’re also the most commonly reported perimenopause symptoms.
A 2023 review in Current Psychiatry Reports identified verbal learning and verbal memory as the cognitive functions most consistently affected during perimenopause, alongside processing speed and attention.1,2
You might be reaching for a word mid-presentation and finding nothing. Losing the thread in a meeting you would have led without notes two years ago. Re-reading the same paragraph. Not forgetting appointments, but spending significantly more cognitive effort to stay on top of what used to run automatically. For senior women, this perimenopause work performance gap is private and rarely named.
The prefrontal cortex and hippocampus are both running in a less stable hormonal environment. Your brain hasn’t been damaged, but it is temporarily recalibrating.1 Most data suggest perimenopause brain fog is most pronounced in early to late perimenopause and stabilizes in postmenopause.
Fatigue is one of the most reported and least explained symptoms. Research has shown that the brain cells, neurons, are generating less energy.11 Estrogen regulates energy production in neurons. When estrogen fluctuates, brain energy metabolism becomes less efficient, which may partly explain you feeling depleted that rest doesn’t restore.
This is not low motivation or poor time management. You’re producing the same output (e.g. the presentation, the decision, the back-to-back calls) on a system running at reduced capacity. The output looks the same. The cost to produce it is substantially higher.
Perimenopausal women have a 40% higher likelihood of developing depressive symptoms than premenopausal women, with risk peaking in early perimenopause.3 Many women with no prior mood history report new-onset anxiety linked to estrogen’s role in serotonin and GABA signaling in the brain, both of which stabilize mood and stress response.4
The hypothalamic-pituitary-adrenal (HPA) axis governs your cortisol stress response and interacts directly with estrogen. As estrogen fluctuates, HPA axis becomes more sensitive to stress, the emotional baseline can move and a routine morning can feel like it’s already too much before 9am.
Irritability, emotional reactivity, feeling wired and depleted at the same time are not character changes. They are downstream effects of your neurological system recalibrating.
A 2025 review found up to 60% of perimenopausal women report some form of sleep disturbance.5 Hot flashes are part of it, but progesterone is the bigger story. Progesterone is converted to neurosteroids that bind to GABA receptors in the brain, helping you fall asleep and get a good night’s sleep. As progesterone declines, calming support weakens. Estrogen fluctuations also disturb circadian rhythm regulation and are associated with altered melatonin production, further destabilizing sleep.6
Perimenopausal fatigue and sleep disruption compound each other, which is why treating the fatigue without addressing the sleep, or vice versa, rarely works.
If you’re noticing these changes, “Am I in perimenopause?” is the right question to be asking.
The most iconic menopause symptom, a hot flash, is a brain event like many others on the list.
In the hypothalamus sits a population of neurons called KNDy neurons. During the reproductive years, estrogen keeps their activity in check. When estrogen falls, KNDy neurons become hyperactive, which is thought to help drive hot flashes and other vasomotor symptoms.9
Hyperactive KNDy neurons send signals to the brain’s temperature control center in the hypothalamus. The brain mistakenly thinks your body is overheating, even though nothing has actually changed. So it triggers a cooling response: blood rushes to the skin and you start sweating. That is a hot flash. It starts in the brain, driven by specific neurons reacting to estrogen loss. The ovaries are not directly involved.
Night sweats are the same mechanism occurring during sleep. Hot flashes and sleep disruption both start in the brain.
Many of the perimenopause symptoms originate in the brain. But estrogen receptors exist throughout the body, and those tissues respond to declining estrogen too. These symptoms tend to arrive later in the transition.
Irregular periods are a hallmark of perimenopause. The most common early change is a shortening of the cycle before they lengthen and become unpredictable. Many women are well into perimenopause neurologically before cycles change at all.7
Joint and muscle pain reflects estrogen’s anti-inflammatory role. As levels fluctuate and fall, connective tissue loses flexibility and inflammation increases. You might experience morning stiffness, aching knees or hips, hands that feel stiff.
Vaginal and urogenital changes such as dryness, discomfort during sex, frequent urination result from estrogen receptor loss in pelvic floor and bladder tissue. These worsen progressively in postmenopause without treatment.
Drier skin and thinning hair reflect estrogen’s role in collagen production and hair follicle cycling. These symptoms are often what prompts women to search ‘Is this menopause?’ for the first time.
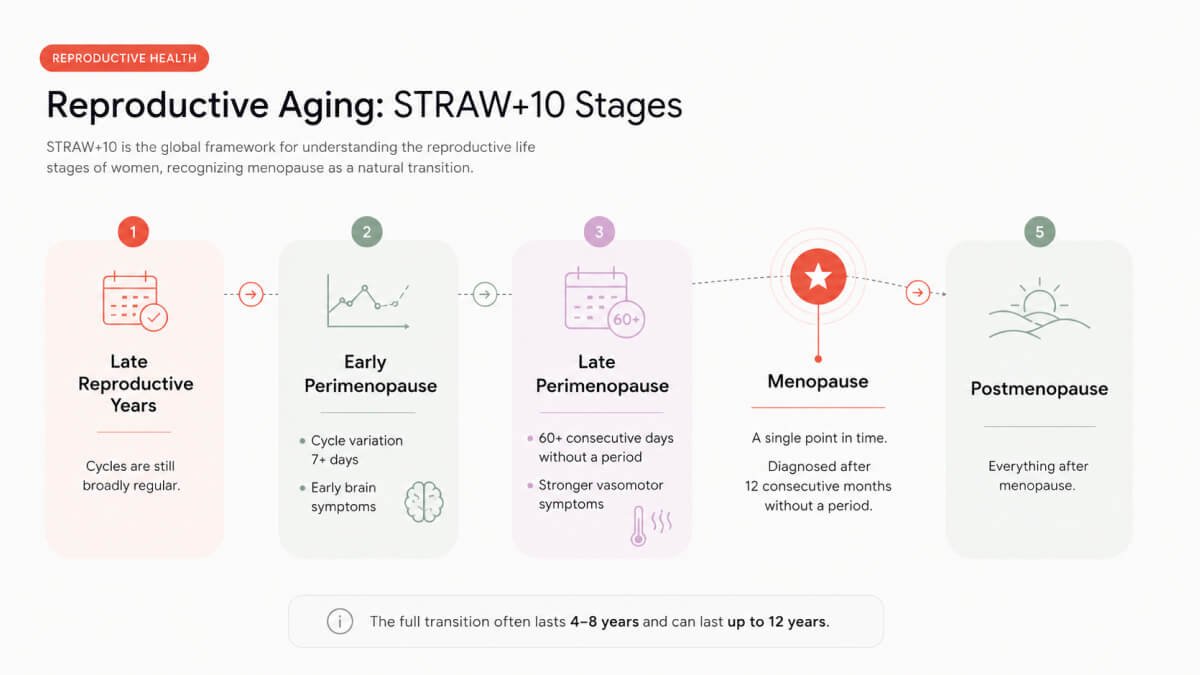
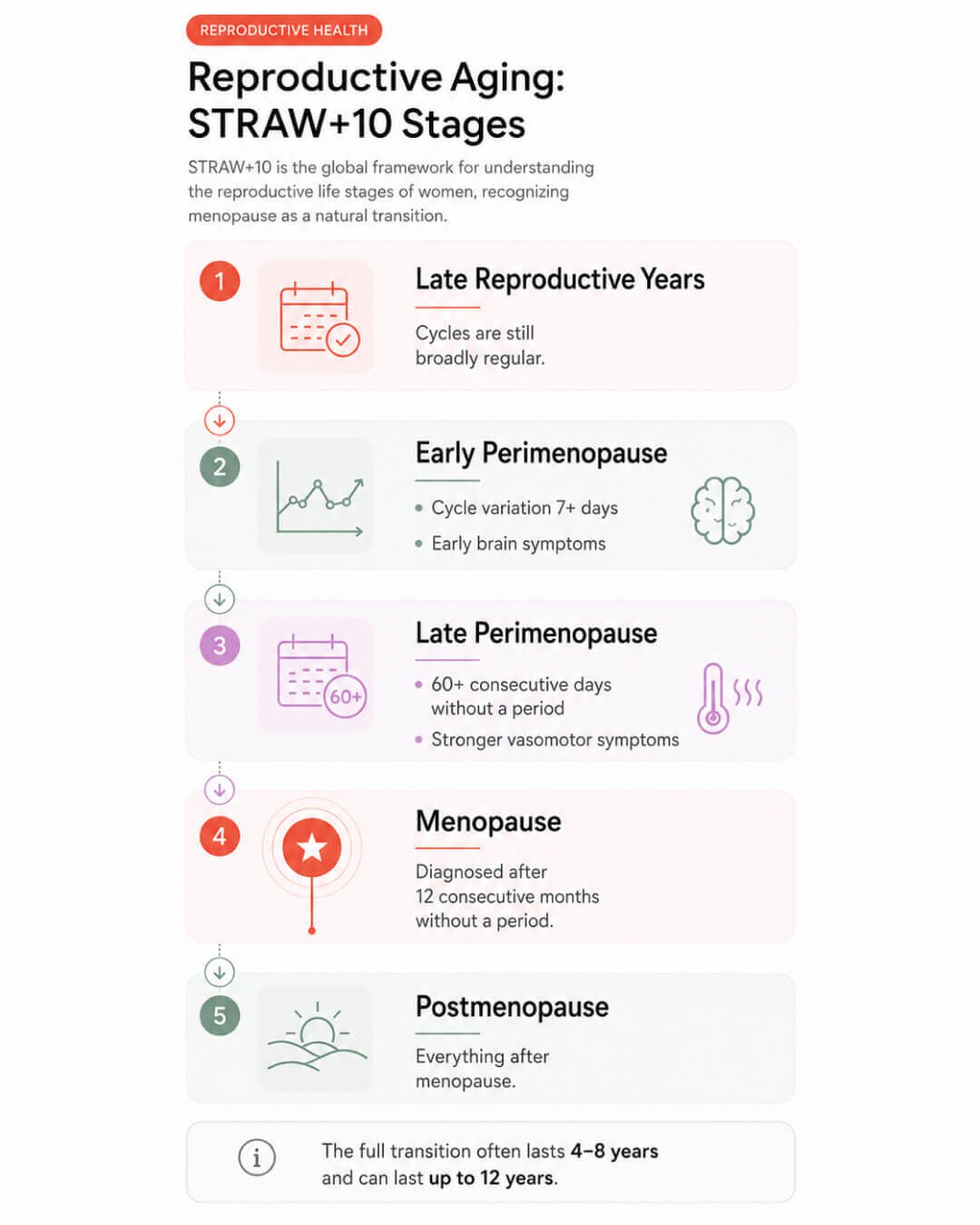
The Stages of Reproductive Aging Workshop (STRAW+10) is the international scientific framework for staging the menopausal transition.7 Most clinicians use it, but not all family docs would know it well. Most women have never even heard of it.
Your menstrual cycle starts to vary, with a difference of 7 days or more between cycles. Cycles often shorten first. FSH starts to rise but fluctuates too widely for a reliable diagnosis. Brain-related symptoms often start before this has even stage begun (and there are many of them!)
60 or more consecutive days without a period, typically lasting one to three years. Vasomotor symptoms are most intense here.
One day in your life. It’s diagnosed after the fact: 12 months in a row without a period. Everything before that point, including the years of brain symptoms, was perimenopause.
The full transition spans roughly 4 to 8 years but can last 12. Most women enter it in their mid-to-late 40s, some in their late 30s.
The question “Am I in perimenopause?” doesn’t require a lab test to answer. The STRAW+10 guidelines are clear: if you’re 45 or older and have typical symptoms and cycle changes, diagnosis is based on your age and symptoms.7
FSH is often tested anyway. The problem is that estrogen swings a lot in early perimenopause, so one FSH result can be misleading. It can be high one week and normal the next.7 FSH testing is more useful under 40, where doctors need to rule out other causes like thyroid issues, premature ovarian insufficiency, or pregnancy.
The most reliable signals are simple when you look at them together: your age (usually 40+), changes in your cycle, and symptoms, especially those affecting your brain and nervous system. You don’t need a formal diagnosis to start taking this seriously.12
These terms are often used as if they mean the same thing, but they don’t.
Perimenopause is the transition. The years when hormones fluctuate and symptoms begin.
Menopause is one point in time. It’s diagnosed after 12 consecutive months without a period.
Postmenopause starts the day after that and continues for the rest of your life.
This distinction matters because symptoms change across these phases. Brain fog and sleep issues are most noticeable during perimenopause. Hot flashes tend to peak later, around late perimenopause and early postmenopause. Bone loss speeds up after your final period.
Asking “am I in perimenopause?” is not hypochondria. It’s pattern recognition.
If you’re in your 40s and have been blaming everything on stress: the word that disappears mid-sentence, the 3am wake-up, the anxiety that came out of nowhere, there’s a good chance perimenopause is part of the picture.
The biology is not subtle: your hippocampus, a memory center, has estrogen receptors. Your sleep depends in part on progesterone. Hot flashes are generated in the brain. And that constant fatigue links to real changes in how your brain produces energy.
Putting a name on it doesn’t fix it. But knowing it’s real, brain-based, and temporary changes how you deal with it.
Dr. Jura Lasas
1.
Metcalf, C. A. et al. Cognitive Problems in Perimenopause: A Review of Recent Evidence (2023) https://doi.org/10.1007/s11920-023-01447-3
2.
Bangle, A. et al. Cognitive Functioning in Perimenopause: An Updated Systematic Review and Meta-Analysis (2026) https://doi.org/10.1037/pag0000946
3.
Badawy, Y. et al. The risk of depression in the menopausal stages: A systematic review and meta-analysis (2024) https://doi.org/10.1016/j.jad.2024.04.041
4.
Jett, S. et al. Ovarian steroid hormones: A long overlooked but critical contributor to brain aging and Alzheimer’s disease (2022) https://doi.org/10.3389/fnagi.2022.948219
5.
Troìa, L. et al. Sleep Disturbance and Perimenopause: A Narrative Review (2025) https://doi.org/10.3390/jcm14051479
6.
Haufe, A. et al. The role of ovarian hormones in the pathophysiology of perimenopausal sleep disturbances: A systematic review (2022) https://doi.org/10.1016/j.smrv.2022.101710
7.
Harlow, S. D. et al. Executive Summary of the Stages of Reproductive Aging Workshop + 10: Addressing the Unfinished Agenda of Staging Reproductive Aging (2012) https://doi.org/10.1210/jc.2011-3362
8.
Yang, J. L. et al. Estrogen deficiency in the menopause and the role of hormone therapy: integrating the findings of basic science research with clinical trials (2024) https://doi.org/10.1097/GME.0000000000002407
9.
Gombert-Labedens, M. et al. Effects of menopause on temperature regulation (2025) https://doi.org/10.1080/23328940.2025.2484499
10.
Prague, J. K. et al. Neurokinin 3 receptor antagonism rapidly improves vasomotor symptoms with sustained duration of action (2018) https://doi.org/10.1097/GME.0000000000001090
11.
Mosconi, L. et al. Menopause impacts human brain structure, connectivity, energy metabolism, and amyloid-beta deposition (2021) https://doi.org/10.1038/s41598-021-90084-y
12.
Harper, J. C. et al. An online survey of perimenopausal women to determine their attitudes and knowledge of the menopause (2022) https://doi.org/10.1177/17455057221106890

Mood & Energy Solutions

Fatigue Causes & Types
Fatigue Causes & Types

Workplace Strategies

Menopause at Work

Brain Fog at Work

Brain Fog at Work

Is This Perimenopause?
Is This Perimenopause?

Nutrition & Supplements

Workplace Strategies

Menopause Science

Menopause Science

Brain Fog Solutions
We use cookies and similar technologies to ensure the proper functioning of our website, personalize content, provide social media features, and analyze traffic. By clicking “I Agree”, you consent to the use of these technologies.
No results





