22 June 2026
Perimenopause Brain Fog Explained: Why You Can’t Think Straight

Reading time 13 min.

Reading time 13 min.
You used to walk into a meeting holding three different thoughts and could pick them up in any order. Now, you lose your train of thought mid-sentence. The change is real, but when you tell your doctor, they usually just say, “You’re fine; it’s just stress.” Perimenopause brain fog is a documented phenomenon that includes different symptoms under one umbrella. Over two-thirds of women notice changes in memory and focus, and it affects everything from work to sleep. The neuroscience here is moving fast, we’ve learned more in the last five years than in the previous fifty.
Perimenopause brain fog is not just one symptom. It covers three areas of thinking that change the most: finding your words mid-sentence, processing speed (how fast you think on your feet), and attention. One large analysis pooled 26 studies with more than 9,000 women. Perimenopausal women scored moderately worse on cognitive tests than premenopausal women. The effect was clearest in studies that carefully defined which stage of the transition women were in.1
The picture gets confusing here. Many women feel a clear cognitive change while their cognitive test scores look normal. Across 24 studies and more than 5,000 women, the link between what women report experiencing and how they score on cognitive tests is weak.2 That mismatch does not mean perimenopause brain fog is imagined. It means the standard tests, designed to catch dementia-level problems, miss the smaller losses women are actually noticing. Your brain compensates by working harder to keep the same output going. The cost is hidden in how much effort it takes to produce the same memo or run the same meeting like before.
Not every woman experiences perimenopause brain fog the same way. Some show clear weaknesses in finding words and recalling information. Others show strengths in attention or complex judgment. Some look entirely typical on tests. It’s so variable that knowing your individual pattern matters more than blanket reassurance.
Estrogen is not only a reproductive hormone. If you are a female, it partly runs your brain. Estrogen receptors are densely packed in the regions that handle memory, attention, and complex judgment: the hippocampus (your memory center) and the prefrontal cortex (the part you use for planning and decision-making).
Think of estrogen as a builder. It builds and maintains dendritic spines, the tiny bumps on neurons where one cell connects to another. More spines mean more connections, and more connections mean faster, more flexible thinking. In animal studies, spine density on memory neurons rises and falls with estrogen levels.³
Estrogen also helps neurons take in glucose, their main fuel. It regulates serotonin and dopamine, the brain’s mood and motivation chemicals. And it boosts BDNF, the growth factor neurons need to remain strong and form new memories. When estrogen drops and swings during perimenopause, all of these systems take are affected at the same time. That stacking is what produces perimenopause brain fog.
Your brain makes its own estrogen, separate from your ovaries. Neurons and supporting brain cells (glia) carry an enzyme called aromatase, which builds estrogen on demand from cholesterol or from androgens (the same hormone family that includes testosterone). This brain-made estrogen works right at the synapse, in real time, the moment a memory is being formed. In a 2024 animal study, researchers used a drug to block this brain-made estrogen. The result was striking. Long-term potentiation, the cellular process behind memory formation, failed. Adding estrogen from outside did not rescue it.4 Your brain needs to make estrogen locally, in the moment, to form memories properly. This is part of why replacement pills alone do not always fix perimenopause brain fog the way you might expect.
As estrogen falls during perimenopause, the brain does not simply lose its estrogen signal. It grows more estrogen receptors. In 2024, Mosconi’s group directly measured estrogen receptor density in the living human brain using a PET scan. Perimenopausal and postmenopausal women had more estrogen receptors in key brain networks than premenopausal women. The pattern itself correctly classified all 54 women in the study as pre- or postmenopausal with 100% accuracy.5 However, more receptors in memory regions were linked with worse memory, and more receptors in mood regions tracked with depression. The brain’s attempt to compensate by growing more receptors to catch less available hormone, which may itself become part of cause of perimenopause brain fog.
The brain is like a city running on glucose. Estrogen helps run the power grid. When estrogen falls, the grid gets less stable, and certain regions start using less fuel. In one landmark imaging study of 43 cognitively normal women aged 40 to 60, perimenopausal and postmenopausal women showed measurably lower glucose use in brain regions vulnerable to Alzheimer’s compared to premenopausal women. The drop also was associated with weaker mitochondrial function in other cells. The women felt normal. They tested normal. But, their brains were already running on less fuel.6
A second study from the same group followed 41 women over three years. Gray matter shrank during perimenopause and partly recovered in the postmenopausal years.7 The brain does adapt. But the years of perimenopause brain fog are when the brain is most strained for energy.
For decades, the story of perimenopause brain fog has been about falling estrogen. New research suggests another hormone may matter just as much.
When the ovaries start slowing down, the brain pushes back. The pituitary gland (a small organ in the brain) releases a hormone called follicle-stimulating hormone, or FSH, to tell the ovaries to keep producing eggs. During perimenopause, FSH rises sharply. After menopause, it stays high for the rest of your life.
For a long time, FSH was thought to be just a marker. New evidence says it may also be a driver. In a 2022 mouse study published in Nature, FSH acted directly on neurons in the hippocampus and cortex. It sped up the buildup of amyloid and tau, the two proteins linked to Alzheimer’s, and worsened memory. When researchers blocked the FSH receptor, all of those changes reversed.8 The pattern translates to humans. Among nearly 900 postmenopausal women, higher FSH levels lined up with worse memory and more amyloid in the brain. Statistical analysis showed FSH affected memory by driving amyloid buildup. Estrogen levels in the same analysis showed no clear relationship to amyloid buildup.9
Measuring FSH alongside estrogen may matter for long-term cognitive risk, not just for fertility. And it raises a real possibility. The rising hormone, not the falling one, may be doing more of the damage. The jury is still out.
Women experience perimenopause brain fog differently. Some women move through the transition with mild changes. Others find it derails work, sleep, and relationships. Three risk factors stand out in the research.
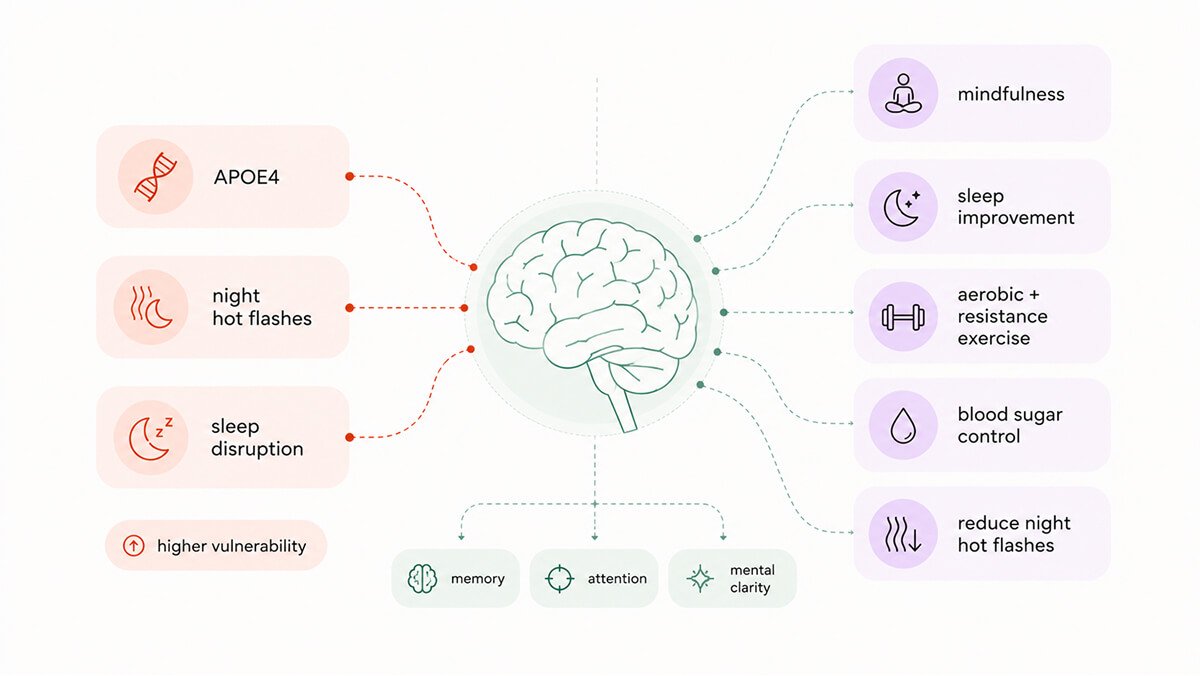
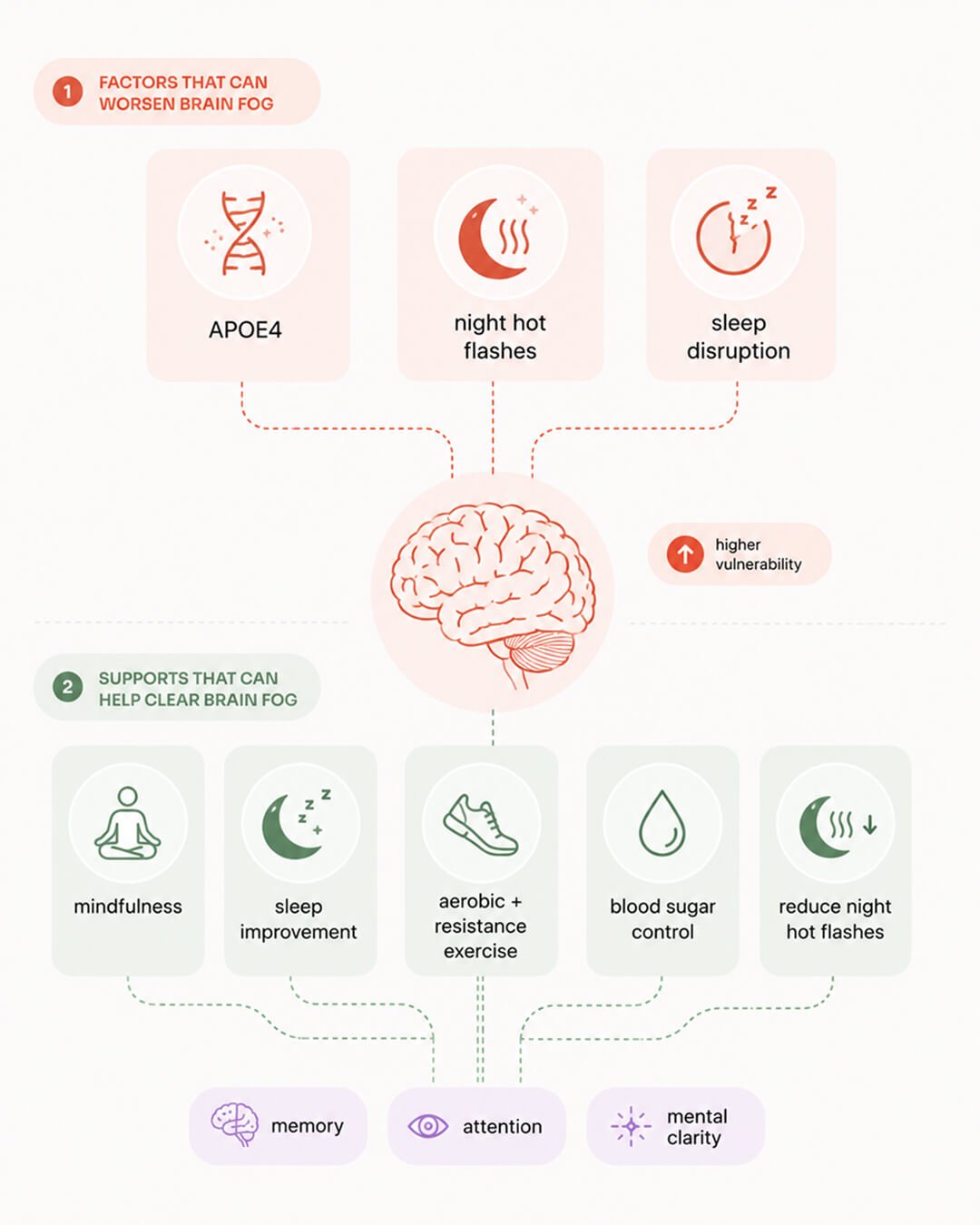
No single intervention fixes everything driving perimenopause brain fog. We would all prefer one, but our biology does not cooperate in this way. The interventions with the strongest evidence each work on a different piece of the picture.
Hormone therapy has a timing-dependent effect on cognition. The critical window hypothesis, supported by observational studies and animal research, says hormone therapy started near the onset of menopause may protect cognition. Starting it a decade later often does not help, and may even cause harm.13 Large randomized clinical trials have not shown a clear cognitive benefit of standard hormone therapy in cognitively healthy women, and current guidelines (both FDA and EMA) do not recommend it specifically for cognitive complaints. One recent finding stands out. In the 2023 EPAD study, HRT was linked to better memory and larger brain volumes specifically in APOE4 carriers, the women at highest genetic risk.14 The finding is promising, but not definitive. Hormone therapy is still a conversation to have with your doctor.
Mindfulness has emerged as the strongest modifiable factor in recent research on perimenopause brain fog. In 2025, researchers analyzed demographic, lifestyle, and symptom factors in more than 200 perimenopausal women. Higher levels of mindfulness were directly linked to having fewer problems with memory and attention. Even after accounting for age, hormone therapy, sleep quality, and other factors, mindfulness remained a significant predictor of better cognitive function.¹⁵ This is not an argument that perimenopause brain fog is psychological. The biology is real. Mindfulness builds attention skills, which may directly counter the focus and decision-making problems driven by lower dopamine and serotonin. It’s a great example of a mind-body connection that we could use to improve our lives.
Sleep, regular aerobic and resistance exercise, blood sugar control, and reducing nighttime hot flashes all work on multiple mechanisms at once. The clinical evidence in midlife women supports each of them, even if the trials specifically in perimenopausal women remain thinner than they should be.
The perimenopause brain fog is not a personality flaw, nor is it early-onset dementia. Recent neuroscience offers a story more complex and more helpful than just “low estrogen.”
The brain is capable of producing its own estrogen, and it even grows more receptors to catch what it can as ovarian levels drop. Furthermore, rising follicle-stimulating hormone (FSH) may be just as impactful as falling estrogen.
While those with the APOE4 gene variant face specific vulnerabilities and may benefit from starting hormone therapy early, most women recover the majority of their cognitive function once the transition is over. The challenges during these years are real, but research into effective solutions is finally gaining momentum.
Dr. Jura Lasas
1.
Bangle, A. et al. Cognitive functioning in perimenopause: An updated systematic review and meta-analysis (2025). https://doi.org/10.1037/pag0000946
2.
Furey, R. T. et al. Subjective versus objective cognition during menopause: A systematic review and meta-analysis (2025). https://doi.org/10.1017/s1355617725101306
3.
Brann, D. et al. Neuron-Derived Estrogen, A Key Neuromodulator in Synaptic Function and Memory (2021). https://doi.org/10.3390/ijms222413242
4.
Maroteaux, M. J. et al. Rapid and local neuroestrogen synthesis supports long-term potentiation of hippocampal Schaffer collaterals-cornu ammonis 1 synapse in ovariectomized mice (2024). https://doi.org/10.1111/jne.13450
5.
Mosconi, L. et al. In vivo brain estrogen receptor density by neuroendocrine aging and relationships with cognition and symptomatology (2024). https://doi.org/10.1038/s41598-024-62820-7
6.
Mosconi, L. et al. Perimenopause and emergence of an Alzheimer’s bioenergetic phenotype in brain and periphery (2017). https://doi.org/10.1371/journal.pone.0185926
7.
Mosconi, L. et al. Increased Alzheimer’s risk during the menopause transition: A 3-year longitudinal brain imaging study (2018). https://doi.org/10.1371/journal.pone.0207885
8.
Xiong, J. et al. FSH blockade improves cognition in mice with Alzheimer’s disease (2022). https://doi.org/10.1038/s41586-022-04463-0
9.
Wang, S. M. et al. Follicle-stimulating hormone linked to cognitive decline and amyloid burden in postmenopausal women (2026). https://doi.org/10.3389/fnagi.2025.1697255
10.
Wang, T. et al. Accelerated midlife endocrine and bioenergetic brain aging in APOE4 females (2025). https://doi.org/10.3389/fnagi.2025.1632877
11.
Thurston, R. C. et al. Menopausal Vasomotor Symptoms and White Matter Hyperintensities in Midlife Women (2022). https://doi.org/10.1212/wnl.0000000000201401
12.
Thurston, R. C. et al. Menopausal Vasomotor Symptoms and Plasma Alzheimer’s Disease Biomarkers (2023). https://doi.org/10.1016/j.ajog.2023.11.002
13.
Maki, P. Critical window hypothesis of hormone therapy and cognition: a scientific update on clinical studies (2013). https://doi.org/10.1097/gme.0b013e3182960cf8
14.
Saleh, R. M. et al. Hormone replacement therapy is associated with improved cognition and larger brain volumes in at-risk APOE4 women: results from the European Prevention of Alzheimer’s Disease (EPAD) cohort (2023). https://doi.org/10.1186/s13195-022-01121-5
15.
Zhu, C. et al. Factors associated with subjective cognitive symptoms during the menopause transition (2025). https://doi.org/10.1097/gme.0000000000002651

Mood & Energy Solutions

Fatigue Causes & Types
Fatigue Causes & Types

Workplace Strategies

Menopause at Work

Brain Fog at Work
Brain Fog at Work

Is This Perimenopause?

Is This Perimenopause?

Nutrition & Supplements

Workplace Strategies

Menopause Science

Menopause Science

Brain Fog Solutions
We use cookies and similar technologies to ensure the proper functioning of our website, personalize content, provide social media features, and analyze traffic. By clicking “I Agree”, you consent to the use of these technologies.
No results





