06 January 2026
Best Menopause Supplements: How to Read Labels and Avoid Marketing Traps

Reading time 11 min

Reading time 11 min
You’re awake at 3 a.m. The night sweat that woke you is starting to lift, but your shirt and sheets are wet and you’re already on your phone. Your husband is breathing too loudly. You hate him for it, briefly, and then you hate yourself for hating him. By 3:30 the social media algorithm has found you. The menopause supplements market lights up your screen in soft pink packaging. Gummies, patches, powders, tinctures, adaptogen blends. They promise hormone balance, restored sleep, lifted brain fog, they promise you the woman you used to be. Some have “OB/GYN Recommended” stamped on the bottle.
You’re trying to figure out which are the best supplements for menopause, but most labels are designed to make that nearly impossible.


Supplements are regulated as food. Medicines are regulated as medicines. The two regulatory worlds have nothing to do with each other.
In 1994 the U.S. Congress passed the Dietary Supplement Health and Education Act, known as DSHEA. The law created a separate framework for supplements and explicitly removed the requirement to prove safety or efficacy before bringing a product to market.¹ A pharmaceutical company developing a new menopause drug runs years of randomized clinical trials, submits the data, and waits for review. A supplement company can formulate a product, design the bottle, and ship it to retailers. There is no efficacy or safety review before the product hits the shelf.
The U.S. Food and Drug Administration can act against a supplement only after it is on the market and only after demonstrating that the product is unsafe.2 Most of us believe supplements are tested and approved by some agency before they appear on the shelves. Studies of consumer beliefs have shown the same misconception: people read “FDA-regulated” and assume “FDA-approved.”3
The supplement market in 1994 had about 4,000 products. It now has over 80,000 and generates roughly $60 billion a year in the U.S. alone.⁴ The regulatory infrastructure has not kept up. The FDA and EMA do not have the inspectors or the laboratories to verify what is in most of these products, and inspections of manufacturing facilities have repeatedly turned up violations of basic quality standards.5
This is why many supplements for menopause and supplements for perimenopause reach the market without strong evidence.
Curious Fact. In 2024, researchers bought 44 weight-loss supplements from retailers on and around U.S. military bases and tested them in a laboratory. Of the 44 products, 82% had inaccurate labels, 91% scored a “no-go” for safety on the Department of Defense’s Operation Supplement Safety scorecard, and none carried a third-party certification seal.6 Weight-loss supplements are a different category, but they sit on the same regulatory shelf as menopause products and are often produced by the same companies. There is no reason to assume the menopause aisle is cleaner.
Companies know that women in their forties and fifties are searching, often desperate, often poorly served by their own clinicians. The market has expanded into that gap.
Within that regulatory frame, brands have developed a specific vocabulary. Companies cannot say “reduces hot flashes” on the bottle. That would require clinical trial data and FDA or EMA approval. So they say something like, “Supports temperature regulation during midlife” or “Promotes hormonal balance” or “Encourages wellness through the menopause transition.”
These are called structure-function claims. The law allows them as long as the company does not name a specific disease or symptom they intend to treat. The wording is designed to imply benefit without ever claiming benefit.
When a brand says “contains clinically studied ingredients,” they are usually not saying their supplement was studied. They are saying that somewhere, sometime, someone studied one of the ingredients in their bottle. The actual product on your kitchen counter has likely never been tested in any controlled setting.
Then there is the dose problem. A study might show that 300 mg of ashwagandha at standardized concentration reduces stress markers. A brand adds 30 mg to its blend. That amount is enough to print “Contains Ashwagandha” on the front of the bottle and nowhere near the dose tested in the study. The industry calls this fairy dusting. You can see it everywhere in the menopause aisle.
When a label boasts a “proprietary blend,” fairy dusting is the most likely reason. A proprietary blend lets a company list ingredients without disclosing how much of each is in the bottle. You see the word “ashwagandha.” You do not see the milligrams. The ingredient might be present in a clinically meaningful dose. It might also be present in a sprinkle.
Reading the label is the only protection you have, and the label is written by the company.
When I evaluate a menopause supplement, I start with one question. What evidence exists for this product? I look at the evidence behind the bottle, not the brand story or the packaging.
The framework I use looks like a pyramid with four tiers. Each tier corresponds to a different strength of evidence. The higher the tier, the more confidence you can have that the menopause or perimenopause supplement might do what the bottle implies. I think of the levels as the four Ps: Proven, Probable, Possible, and Pretend.
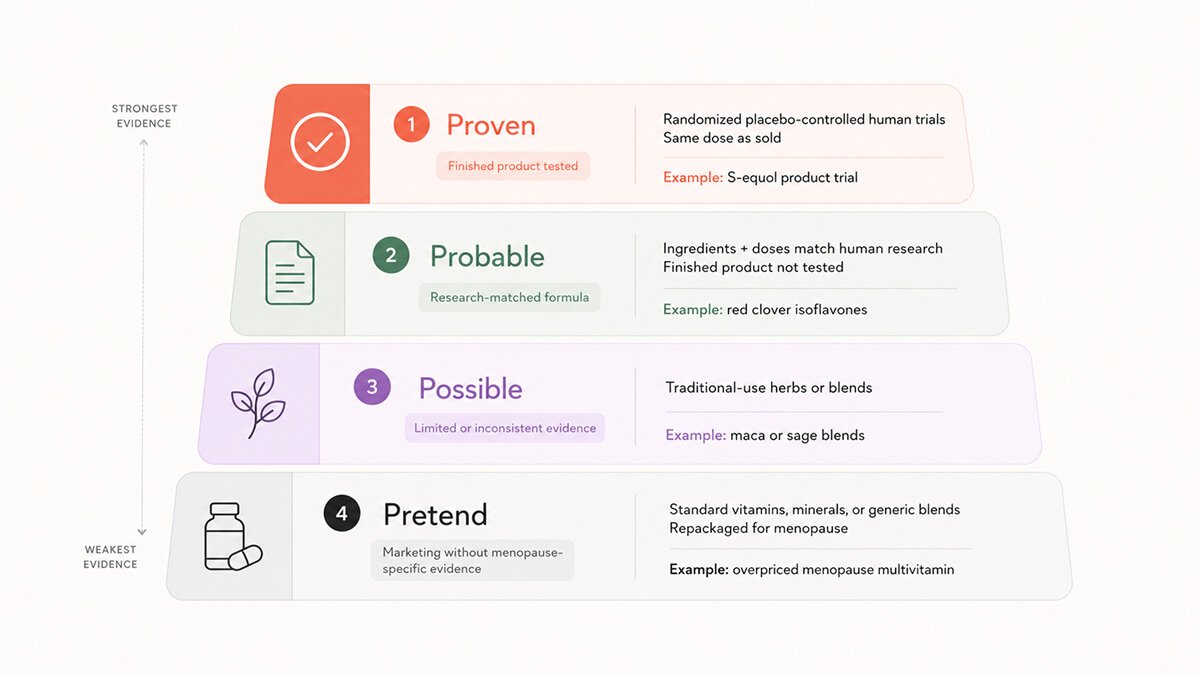

The company has paid for randomized placebo-controlled trials on the supplement you are about to buy. Not on the ingredient in general. On the actual finished product, in the dose and combination they sell.
Tier 1 is rare. A clinical trial costs millions of dollars and the company is not legally required to do one. When a brand has invested in Tier 1 evidence, they usually make it easy to find. They publish the trial on their website, cite the trial registration number, and name the journal.
Bonafide Health sells Equelle, a supplement built around S-equol, a metabolite of the soy isoflavone daidzein. The supplement was tested in a randomized placebo-controlled trial of 160 postmenopausal women. After 12 weeks, the S-equol group had a 58.7% reduction in daily hot flash frequency compared with a 34.5% reduction in the placebo group.7 Even though the trial was small, it was on the actual product and at the actual dose.
If a brand has run a Tier 1 trial, they care about evidence. They are very rare in the menopause supplement aisle, but these are the closest you will get to the best supplements for menopause based on real clinical evidence.
The brand did not test its finished product. They built it using ingredients and doses that have been tested by others.
Tier 2 brands are relying on established science. The assumption that their formulation behaves the same way is an assumption.
Red clover isoflavones are a useful example. Pooled analyses of eight trials show a statistically significant reduction in daily hot flashes among women receiving red clover compared to placebo, with the strongest effects appearing at doses of 80 mg or more per day taken for at least 12 weeks.8 Promensil uses 80 mg of red clover isoflavones standardized for biochanin A content, the same range the trials evaluated. Promensil itself has not been tested as a finished product in a large trial, but the dose and the ingredient match the published evidence.
The catch with Tier 2 is the dose. A brand that uses an ashwagandha extract at the same dose used in published research is Tier 2. A brand that hides a fraction of that dose inside a “proprietary blend” is something else.
Many of the best supplements for menopause fall into this category when dosing matches research.
Traditional medicine systems have used the herb for generations. The evidence of traditional medicine use for menopause or perimanopause symptoms is too inconsistent to call it probable.
Tier 3 holds such menopause supplements as chasteberry, maca, sage, wild yam, and most of the “balance blends” that combine several of them at low doses. They might help. They might not. Mechanism research, when there is any, points to weak estrogenic activity or general anti-inflammatory effects rather than a specific pathway in menopause physiology.9
The Health & Her Perimenopause Multi-Nutrient is a useful Tier 3 example. The product bundles maca, sage, ginseng, and red clover, with red clover sitting at a Tier 2 dose and the other three at Tier 3 traditional-use levels. The brand has a strong social media presence and powerful customer testimonials on using it as a perimenopause and menopause supplement. The finished product has not been tested in a randomized trial for perimenopausal symptoms.
Tier 3 is the territory where the placebo effect, regression to the mean, and genuine mild benefit all blur together. Some women feel better on Tier 3 menopause supplements. Some of that effect is real, even if the mechanism is non-specific. Some of it is the powerful expectation that comes from spending money and committing to a routine.
If you want to try a Tier 3 product, do it with realistic expectations. Modest, inconsistent, possibly placebo-driven, possibly real. Most over-the-counter perimenopause supplements sit in this tier.
Generic vitamins and minerals, repackaged with menopause language and sold at three to five times the cost of the same ingredients on the same shelf, are the easiest available menopause supplements.
Tier 4 examples are vitamin D, vitamin B6, magnesium, omega-3, and standard multivitamin formulations. They are put in a pretty bottle, with the word “Menopause” on the label, and charged accordingly. You may genuinely need vitamin D or magnesium. The deception sits in the implied specificity to menopause.
Several physician-branded menopause supplement lines marketed to midlife women fall into this tier. Independent testing services that compare ingredient lists and prices to comparable products on the same shelves repeatedly find that the menopause-positioned formulation is essentially a standard multivitamin with target-audience marketing.10
There is nothing wrong with taking a multivitamin. Buy a generic one for fifteen dollars or euros instead of a branded one for eighty.
This is one of the most common categories of supplements for menopause sold online.
The cognitive menopause supplements category is where the menopause market is moving fastest. Brain fog has become the perimenopause symptom most likely to threaten a woman’s career. Forgetting a name in a meeting. Losing a thread mid-presentation. Walking into a room and not remembering why. The market for “cognitive support” and “focus” supplements has expanded into that fear.
Soy isoflavones, the most studied phytoestrogens, have produced inconsistent results in cognitive trials. The systematic reviews to date have not been able to conclude that isoflavones reliably improve cognition or urogenital symptoms.11 Some studies show small improvements in verbal memory in women within ten years of menopause. Most do not.
Resveratrol has a stronger signal. In postmenopausal women, supplementation with 75 mg of trans-resveratrol twice daily over 24 months produced a 33% improvement in overall cognitive performance compared to placebo, along with measurable improvements in brain blood flow.12 Resveratrol acts on the vascular endothelium and improves blood flow to the brain, which matters more after menopause when estrogen-driven vascular protection has decreased. The dose used in the trial is high. Several of the published trials are funded by the supplement industry, which is worth knowing.
Creatine is the newest entrant. Most creatine research has been done in athletes and older adults, but emerging trials in perimenopausal and postmenopausal women have started to fill the gap. In one randomized controlled trial of 36 women, medium-dose creatine hydrochloride at 1,500 mg per day over 8 weeks improved reaction
time and increased frontal brain creatine concentrations compared to placebo.13 The trial is very small, but the mechanism is interesting. Creatine supports cellular energy metabolism in the brain, and brain energy metabolism is one of the better-documented changes in the menopause transition. More research is coming.
The honest summary. Most cognitive menopause supplements are Tier 3. A handful (resveratrol and creatine) are in Tier 2 territory based on mechanism and emerging trials. None of them, on the current evidence, will restore the cognitive baseline you had at 35.
When you see these phrases, slow down. They almost always signal Tier 3 or Tier 4 territory.


“Hormone-free HRT alternative.” Hormone replacement therapy replaces estrogen, progesterone, and testosterone. Supplements cannot replace hormones. The phrase is engineered to play on hormone fear and promise hormone outcomes.
“Balances hormones naturally.” “Hormonal balance” is not a measurable medical concept. There is no test for it. The phrase is a marketing artifact, not a physiological state.
“Detoxifies excess estrogen.” Your liver and kidneys do detoxification continuously and competently. They do not need a supplement.
“Proprietary blend.” This phrase means the company is not telling you how much of each ingredient is in the bottle. Treat it as missing data.
“Clinically studied ingredients.” This phrase usually means an ingredient was studied somewhere by someone, not that the actual product was studied.
“Clinically validated formula.” Without a peer-reviewed paper on the actual formula, the phrase is decorative.
“#1 OB/GYN recommended.” There is no central body that ranks supplements by gynecologist recommendation. The phrase is invented.
“100% natural, therefore safe.” Mercury is natural. Hemlock is natural. Some menopause herbs interact with medications and affect liver enzymes. Natural is not a synonym for safe.
“Targets the root cause of menopause.” The root cause of menopause is your ovaries running out of follicles. No supplement reverses that.
“Targets the 34 symptoms of menopause.” No supplement has been shown to address most of the symptoms attributed to menopause. The number 34 itself comes from a marketing infographic, not a clinical guideline.
“Doctors don’t want you to know about this.” Conspiracy framing. Skip.
“Empower your wellbeing.” Designed to feel inspirational while saying nothing.
“As featured in [major media outlet].” A journalist mentioning a brand in an article is not scientific evidence.
The pattern across all of these is the same. The phrase sounds medical, sounds specific, and falls apart when you try to convert it into a measurable claim.
These phrases are common across both supplements for menopause and perimenopause.
The framework I just walked you through helps you tell a useful supplement from a useless one. It cannot help you tell a useful supplement from one that fixes the underlying biology. The truth is none of them do.
The biological event of menopause is the depletion of ovarian follicles. Estrogen production falls off, gradually then sharply, and the systems that depended on estrogen for over thirty years have to adapt. The brain has to adapt. The vasculature has to adapt. Bone density, glucose metabolism, sleep architecture all have to adapt. The woman doing the adapting has to keep going to work, raise the children, and run the teams or companies.
Menopause supplements are not useless. A well-chosen Tier 1 or Tier 2 product can take the edge off specific symptoms, and that matters when you are trying to function at the level your career requires. The bottle is one piece of a puzzle that includes your sleep, your training, your protein, your relationships, and in many cases your access to a clinician who actually understands midlife endocrinology.
Reading the label like a scientist is a defense. It is not the whole answer.
There is a place for menopause supplements in midlife care. The problem is the vague language brands use to sell them. I am in perimenopause myself. I read these labels for myself and for the women I write for.
The framework I have walked you through is a defense against predatory marketing. A Tier 1 or Tier 2 menopause supplement at the right dose can take the edge off specific symptoms. Do not confuse that with fixing the biology underneath.
Dr. Jūra Lašas
1.
Bailey, R. Current regulatory guidelines and resources to support research of dietary supplements in the United States. Critical Reviews in Food Science and Nutrition (2018). https://doi.org/10.1080/10408398.2018.1524364
2.
Frankos, V. et al. FDA Regulation of Dietary Supplements and Requirements Regarding Adverse Event Reporting. Clinical Pharmacology & Therapeutics (2010). https://doi.org/10.1038/clpt.2009.263
3.
Dodge, T. et al. Influence of the Dietary Supplement Health and Education Act on Consumer Beliefs About the Safety and Effectiveness of Dietary Supplements. Journal of Health Communication (2011). https://doi.org/10.1080/10810730.2010.529493
4.
Wallace, T.C. et al. DSHEA 1994: Celebrating 30 Years of Dietary Supplement Regulation in the United States. Journal of Dietary Supplements (2024). https://doi.org/10.1080/19390211.2024.2419434
5.
Marcus, D. Dietary supplements: What’s in a name? What’s in the bottle? Drug Testing and Analysis (2016). https://doi.org/10.1002/dta.1855
6.
Crawford, C. et al. Label Accuracy and Quality of Select Weight-Loss Dietary Supplements Sold on or near US Military Bases. Nutrients (2024). https://doi.org/10.3390/nu16244369
7.
Aso, T. et al. A Natural S-Equol Supplement Alleviates Hot Flushes and Other Menopausal Symptoms in Equol Nonproducing Postmenopausal Japanese Women. Journal of Women’s Health (2012). https://doi.org/10.1089/jwh.2011.2753
8.
Kanadys, W. et al. Evaluation of Clinical Meaningfulness of Red Clover (Trifolium pratense L.) Extract to Relieve Hot Flushes and Menopausal Symptoms in Peri- and Post-Menopausal Women: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients (2021). https://doi.org/10.3390/nu13041258
9.
Yelland, S. et al. The role of diet in managing menopausal symptoms: A narrative review. Nutrition Bulletin (2023). https://doi.org/10.1111/nbu.12607
10.
Cooperman, T. ConsumerLab’s Review of The ‘Pause Nutrition Supplements by Dr. Mary Claire Haver. ConsumerLab (2024). https://www.consumerlab.com/
11.
Chen, L-R. et al. Isoflavone Supplements for Menopausal Women: A Systematic Review. Nutrients (2019). https://doi.org/10.3390/nu11112649
12.
Thaung Zaw, J.J. et al. Long-term effects of resveratrol on cognition, cerebrovascular function and cardio-metabolic markers in postmenopausal women: A 24-month randomised, double-blind, placebo-controlled, crossover study. Clinical Nutrition (2020). https://doi.org/10.1016/j.clnu.2020.08.025
13.
Korovljev, D. et al. The Effects of 8-Week Creatine Hydrochloride and Creatine Ethyl Ester Supplementation on Cognition, Clinical Outcomes, and Brain Creatine Levels in Perimenopausal and Menopausal Women (CONCRET-MENOPA): A Randomized Controlled Trial. Journal of the American Nutrition Association (2025). https://doi.org/10.1080/27697061.2025.2551184

Mood & Energy Solutions

Fatigue Causes & Types
Fatigue Causes & Types

Workplace Strategies

Menopause at Work

Brain Fog at Work

Brain Fog at Work

Is This Perimenopause?

Is This Perimenopause?
Nutrition & Supplements

Workplace Strategies

Menopause Science

Menopause Science

Brain Fog Solutions
We use cookies and similar technologies to ensure the proper functioning of our website, personalize content, provide social media features, and analyze traffic. By clicking “I Agree”, you consent to the use of these technologies.
No results





