22 June 2026
Early Perimenopause Symptoms Start in the Brain (Before Your Periods Change)

Reading time 9 min.

Reading time 9 min.
You are in your early 40s, at the top of what you can do. And something has changed.
You reach for a word mid-sentence and it’s not there. You leave a meeting you were completely prepared for feeling depleted. You wake at 3am, heart racing, nothing obviously wrong. You feel anxious on a Tuesday morning before the day has even started. Your periods are mostly fine, so you find the logical explanation: too much travel, a brutal quarter, not enough sleep. You cut the wine, add the magnesium, restructure your mornings. Some of it helps a little. None of it fixes the thing you can’t quite name. Many say: “I just don’t feel like myself…”
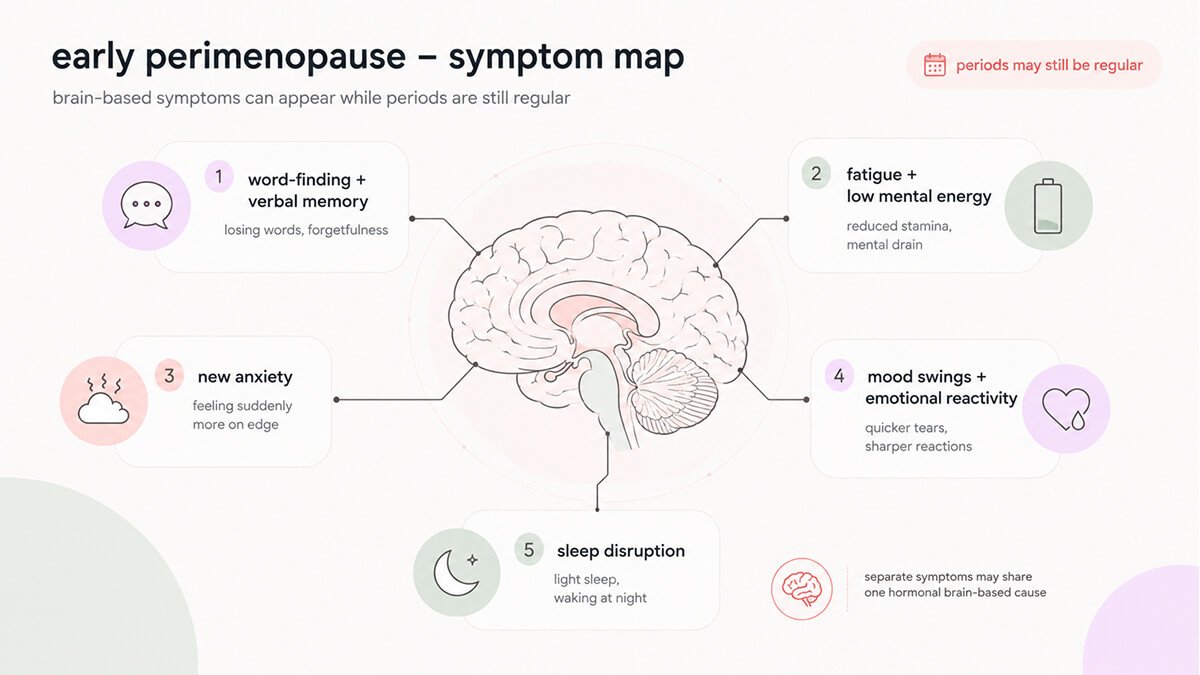
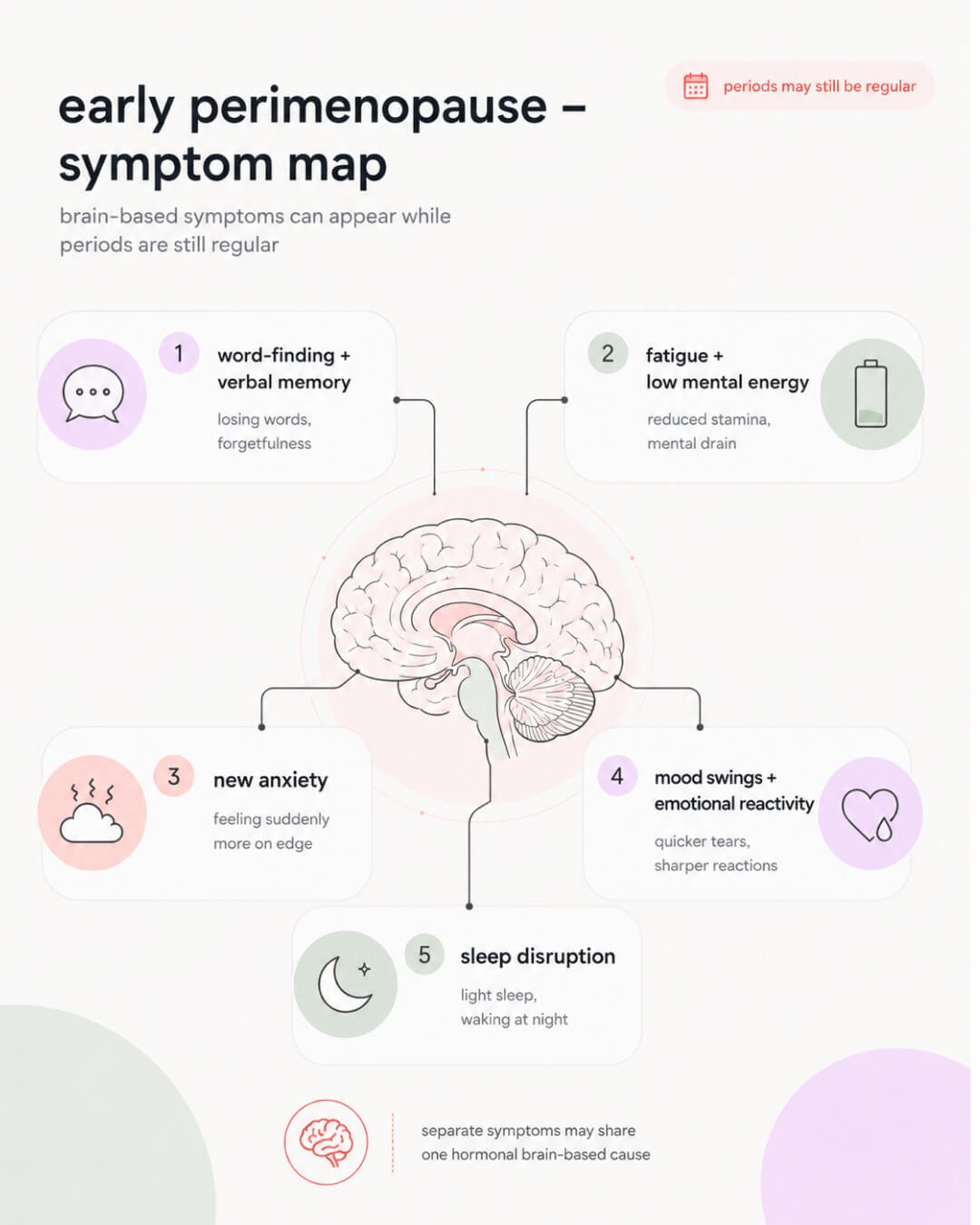
Early perimenopause symptoms are typically neurological, and they arrive before your periods change. Most women don’t know that and it’s why so many high achievers spend months, sometimes years, solving the wrong problem.
You’re mid-sentence in a meeting, and you can’t remember the word “budget.” You’ve used it every week for fifteen years. Instead, you use “money plan,” feeling completely silly and wondering if you are losing it. The word “budget” comes back thirty seconds later, when the moment has already moved on. Research tracking women across the menopausal transition consistently finds that memory retrieval complaints peak during perimenopause itself, not postmenopause. Age isn’t the main driver.1 Word-finding is one of the most common early perimenopause symptoms. The sharper your baseline, the more disorienting it feels.
Fatigue is one of the most commonly missed early perimenopause symptoms because it’s invisible from the outside. You sleep well enough and still feel like you’re pushing through all day. A document you’d normally scan in two minutes needs three reads. You take notes in conversations you used to follow without thinking. The output looks fine from the outside. The internal cost is much higher. Earlier bedtimes don’t fix it, because the cause isn’t how much sleep you’re getting.
The anxiety is the most underlooked early perimenopause symptom most likely to be filed under “life.” You wake up already bracing for a storm. You sit in a meeting feeling like something is about to go wrong, nothing specific, just a low hum of dread underneath. Large longitudinal studies following thousands of women across more than a decade found that women with no prior anxiety history were significantly more likely to develop elevated anxiety specifically during early perimenopause, independently of hot flashes, life events, and financial stress.2 The anxiety wasn’t related to midlife in general, but the hormonal transition specifically.
Mood swings are one of the early perimenopause symptoms that most often goes unnamed. They feel different from anxiety, but they often show up around the same time. Small irritations hit you harder than they used to. And it takes longer to come back from them. You can feel wired and completely drained at the same time, sometimes in the same afternoon. This isn’t you falling apart or reaching your limit. It’s your emotional system trying to function in a neurochemical environment it hasn’t experienced before.
Sleep disruption is one of the early perimenopause symptoms most clearly connected to progesterone decline. You attribute waking at 3am to stress, lying there with your brain already running through tomorrow’s agenda. But progesterone starts declining before periods become irregular. Progesterone supports deep consolidated sleep through its conversion to neurosteroids that bind to GABA receptors in the brain. When progesterone drops, that calming structure weakens.3
Curious fact: Perimenopausal cognitive changes are not uniform. A significant proportion of women experience no meaningful disruption at all. Among those who do, verbal memory and word retrieval are the most commonly affected areas, not global cognitive function, not intelligence, not professional capability.1
Early perimenopause symptoms can appear long before any visible cycle changes. The international scientific staging framework for reproductive aging (STRAW+10) defines early perimenopause as beginning when cycle length starts varying by seven or more days.9 But brain and mood changes don’t wait for that threshold. They tend to start in what researchers call the late reproductive stage, when ovulation becomes less predictable, progesterone begins to drop, and estrogen starts fluctuating. Many brain-related symptoms appear before your cycle shows anything on a calendar. Your brain got the news earlier. Your calendar just hasn’t caught up yet.
Recognizing early perimenopause symptoms is about connecting patterns, not running a single test. There is no blood test that confirms early perimenopause. Follicle-stimulating hormone (FSH) fluctuates too much in the early transition to be reliably read from a single blood draw. Clinicians assess age (typically 40 or above), symptoms, and any cycle changes together. The absence of period changes doesn’t rule out perimenopause. For women who’ve explained every symptom as a work or lifestyle problem, perimenopause is worth considering as the explanation.
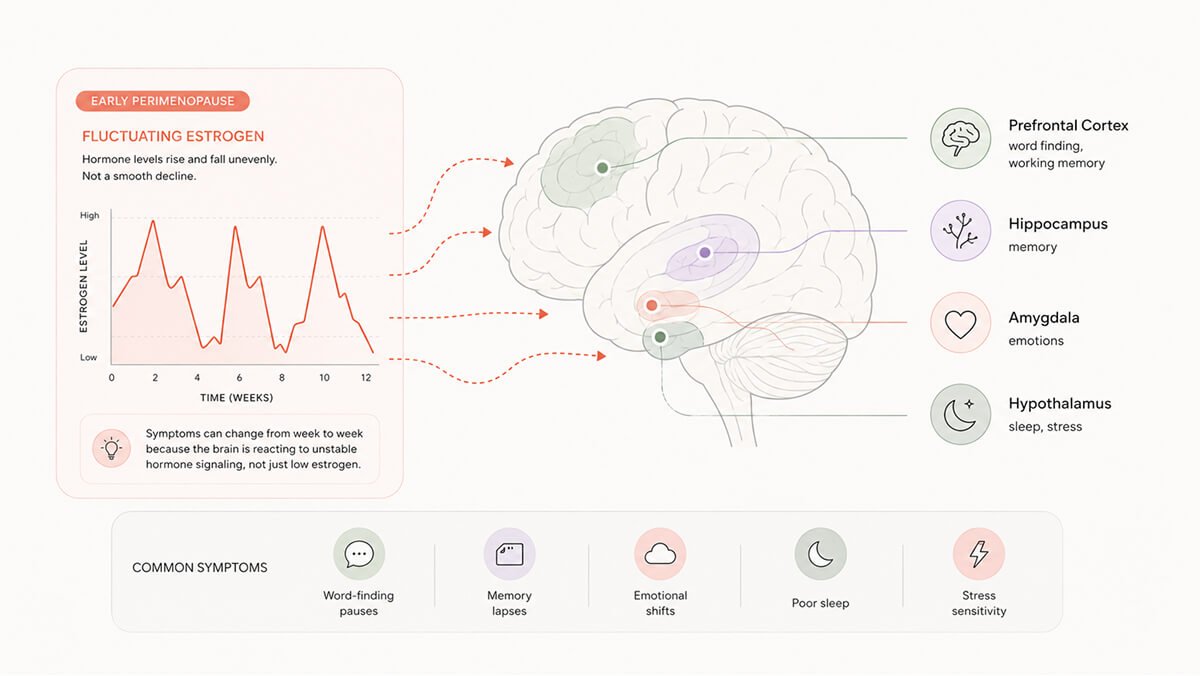
Many early perimenopause symptoms come from the brain, and that’s because estrogen isn’t just a reproductive hormone that occasionally wanders into the brain. It’s a neuromodulator with receptors concentrated across the prefrontal cortex (decision-making, verbal retrieval, working memory), the hippocampus (memory consolidation), the amygdala (emotional processing and threat response), and the hypothalamus (sleep, temperature, and stress regulation). These regions have been actively regulated by estrogen your entire reproductive life. When estrogen levels change, all of them feel it.
In early perimenopause, estrogen doesn’t fall in a straight line. It behaves more like turbulence on a flight: sudden drops, unexpected spikes, sometimes both in the same cycle. The brain’s estrogen-sensitive networks respond to change, not just to low levels. Unpredictable hormone variability is a very disruptive signal to the brain. That’s why you can feel completely fine one week and foggy and anxious the next.10 It’s also a reason why a single blood test on a single day tells you almost nothing useful.
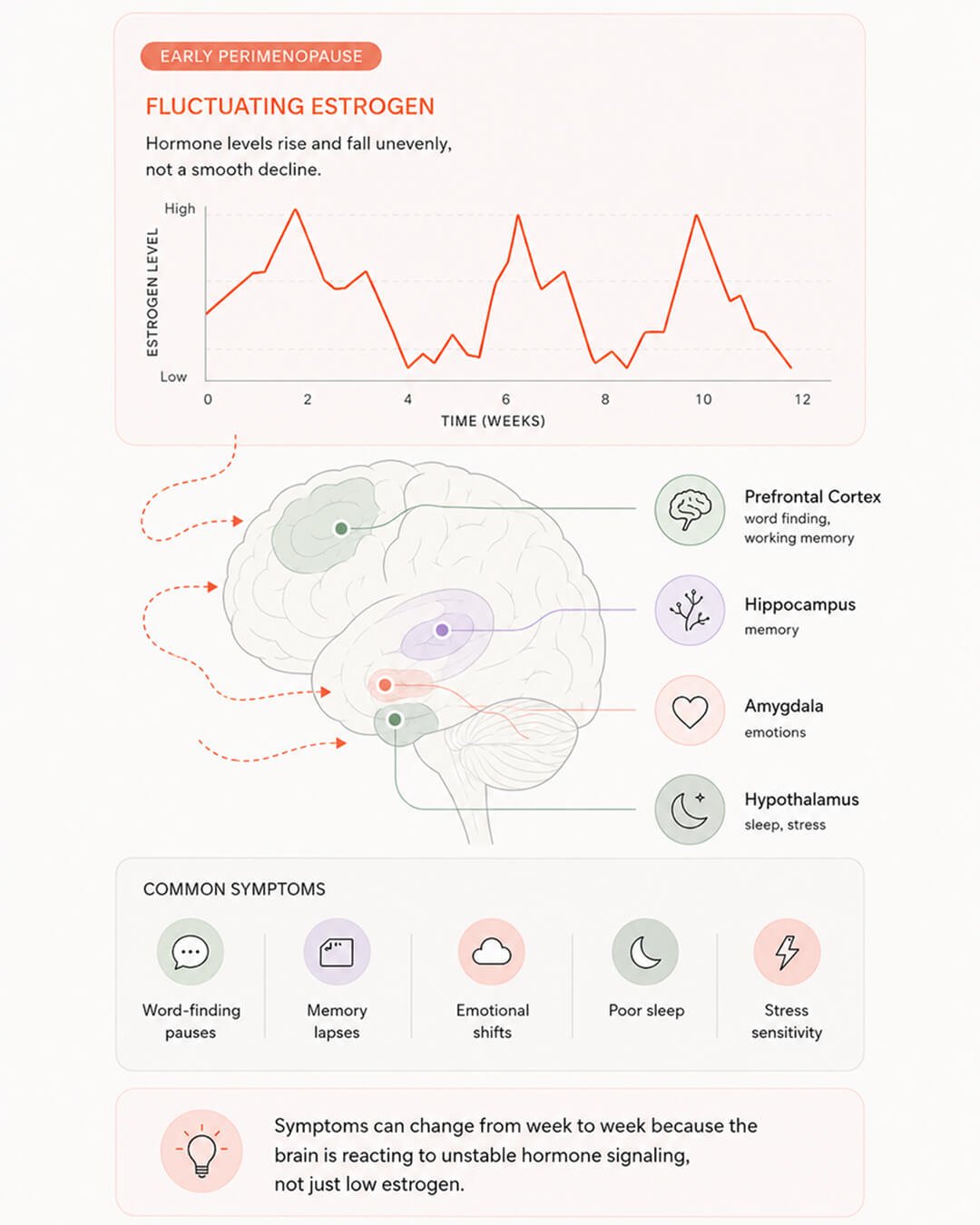
Early perimenopause symptoms can feel unpredictable from week to week because your nervous system loses some of its steadiness. Estrogen and progesterone don’t only regulate your cycle. They also keep your brain’s calming system running. The calming system relies on a neurotransmitter GABA, which tells your brain that a full inbox is just a full inbox, not a threat to react to. When estrogen and progesterone are balanced, GABA signaling is strong, and your reactions match the situation. In perimenopause, the GABA signal weakens. Progesterone drops, estrogen fluctuates, and the brain struggles to settle after small stressors. The same email that used to register as routine now registers as urgent. Recovery takes longer. This isn’t a loss of resilience. It’s a shift in baseline neurochemistry. Your brain working without the calming support it had for decades.
And this isn’t just a feeling or a story we’re telling ourselves. When researchers look at the brain, they can see real changes happening during this transition. They see structural brain changes, the way different areas communicate change, and even how the brain uses energy starts to look different.8 This brain change can’t be attributed to just “getting older” or “being overwhelmed at work.” It’s specifically tied to hormonal changes.
Early perimenopause symptoms reflect real changes in brain function, not just aging. Your brain is running on the same hardware, but the operating system is being updated in the background. Things still work, just not in quite the same smooth, predictable way. And all of this starts before menopause is even officially on your calendar.
Curious fact: When scientists compare women’s brains in perimenopause to men’s of the same age, they don’t see the same changes in men. So this isn’t just about getting older, because if it were, men would show it too. Your brain is adapting to a hormonal shift, not just the passing of time.8
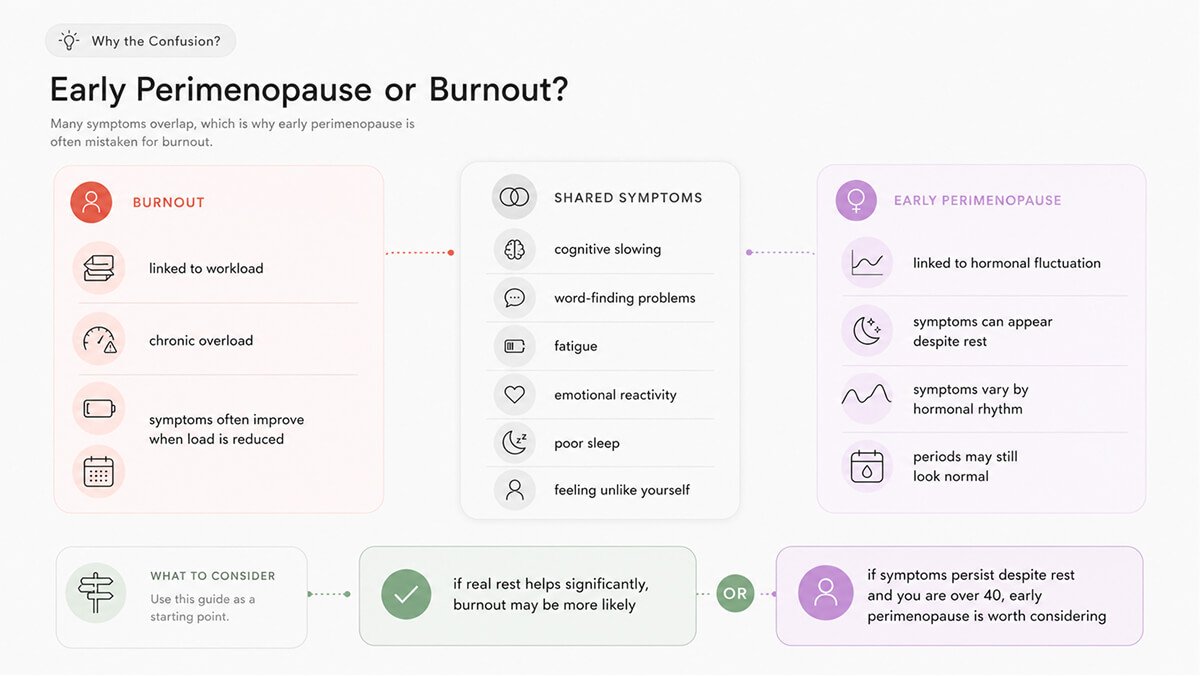
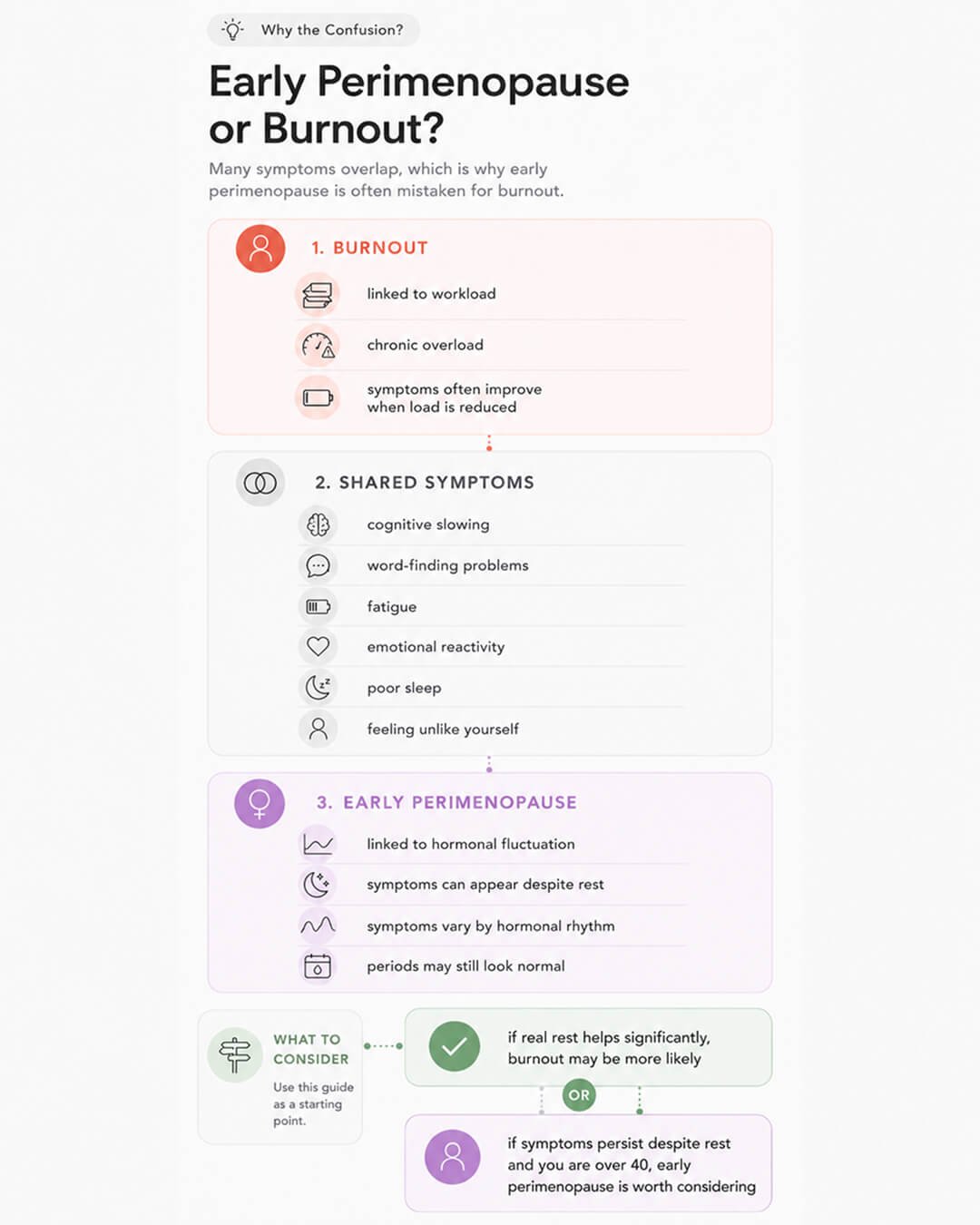
The symptoms between early perimenopause and occupational burnout overlap significantly: cognitive slowing, words going missing, emotional reactivity, fatigue, a sense that you’re not quite yourself at work. For a senior woman in her early-to-mid 40s, burnout is the more plausible conclusion. In a culture that doesn’t talk about perimenopause brain fog, it’s often the only explanation for what you are feeling.
There are documented clinical cases where perimenopausal cognitive symptoms were attributed to early-stage dementia by doctors, not just by the women themselves.4 If that happens in healthcare settings with trained professionals, it’s not surprising that high-performing women reach the same wrong conclusion. Many spend months quietly scaling back, passing on projects, wondering whether something more serious is happening.
One of the clearest ways to tell early perimenopause symptoms apart from burnout is how they respond to rest. Burnout usually gets better when you reduce the load. You rest, you step back, you take a couple of weeks off, and you start feeling better. But perimenopause brain fog doesn’t respond to rest the same way. It’s not coming from overuse, so it doesn’t respond to rest in the same way. It runs on a hormonal rhythm that has nothing to do with how busy you’ve been, and it can still be there on Monday morning even after a genuinely relaxing weekend. So if you’ve actually rested and the mental friction is still there, that’s something to pay attention to.
Many women navigating early perimenopause symptoms misread the experience as a decline in capability. Working women across multiple countries report that perimenopause symptoms are affecting their performance, and many go out of their way to hide the symptoms because they’re worried about how they’ll be perceived at work.5,6 What the numbers don’t capture is the private conclusion many reach: that they’ve hit some kind of ceiling. The ceiling isn’t real. They’re navigating a neurological transition with no name in any leadership program they’ve ever attended.
The research is consistent: early perimenopause symptoms often show up in the brain first.. Slower thinking, new anxiety, words disappearing mid-sentence, mood swings… These aren’t signs that you suddenly can’t handle your workload. They’re early perimenopause signs your brain is trying to function in a hormonal environment it has never had to operate in before.
I know the feeling well, I’m in perimenopause myself. I have changed how I structure my weeks, how I protect my effective hours, and how much I expect from myself on the days that feel heavier.
The most expensive part of early perimenopause symptoms isn’t the symptoms themselves. It’s the silence around them and the wrong stories we tell ourselves to make sense of the changes. If you’re in your early to mid-40s, doing cognitively demanding work, and something has felt consistently off, perimenopause is worth looking into, not as a worst-case scenario, but as the one that finally makes everything click.
Dr. Jura Lasas
1.
Metcalf, C. A. et al. Cognitive Problems in Perimenopause: A Review of Recent Evidence (2023) https://doi.org/10.1007/s11920-023-01447-3
2.
Bromberger, J. T. et al. Does risk for anxiety increase during the menopausal transition? Study of Women’s Health Across the Nation (2013) https://doi.org/10.1097/gme.0b013e3182730599
3.
Troìa, L. et al. Sleep Disturbance and Perimenopause: A Narrative Review (2025) https://doi.org/10.3390/jcm14051479
4.
Thomas, E. et al. Minding menopause in patients with cognitive impairment: a patient’s perspective and reflections on clinical practice (2023) https://doi.org/10.1186/s12905-023-02770-w
5.
Alzueta, E. et al. Navigating menopause at work: a preliminary study about challenges and support systems (2024) https://doi.org/10.1097/GME.0000000000002333
6.
Wood, K. et al. “Hiding symptoms and balancing work, family and relationships”: Australian women discuss menopause and the midlife collision (2025) https://doi.org/10.1016/j.socscimed.2025.118681
7.
Gordon, J. L. et al. Ovarian Hormone Fluctuation, Neurosteroids, and HPA Axis Dysregulation in Perimenopausal Depression: A Novel Heuristic Model (2015) https://doi.org/10.1176/appi.ajp.2014.14070918
8.
Mosconi, L. et al. Menopause impacts human brain structure, connectivity, energy metabolism, and amyloid-beta deposition (2021) https://doi.org/10.1038/s41598-021-90084-y
9.
Harlow, S. D. et al. Executive summary of the Stages of Reproductive Aging Workshop + 10: addressing the unfinished agenda of staging reproductive aging (2012) https://doi.org/10.1097/gme.0b013e31824d8f40
10.
Joffe, H. et al. Impact of Estradiol Variability and Progesterone on Mood in Perimenopausal Women With Depressive Symptoms (2020) https://doi.org/10.1210/clinem/dgz181

Mood & Energy Solutions

Fatigue Causes & Types
Fatigue Causes & Types

Workplace Strategies

Menopause at Work

Brain Fog at Work

Brain Fog at Work
Is This Perimenopause?

Is This Perimenopause?

Nutrition & Supplements

Workplace Strategies

Menopause Science

Menopause Science

Brain Fog Solutions
We use cookies and similar technologies to ensure the proper functioning of our website, personalize content, provide social media features, and analyze traffic. By clicking “I Agree”, you consent to the use of these technologies.
No results





