22 June 2026
Perimenopause Exhaustion: 5 Reasons Why You’re So Tired and What Actually Helps

Reading time 15 min.

Reading time 15 min.
You wake up feeling as though you never slept. You did everything right the night before, dinner was early, the lights were dimmed, and you were in bed at a reasonable hour, yet you feel completely depleted. By mid-afternoon, you no longer have mental energy. While the conversation around menopause usually centers on hot flashes, menopause fatigue is the symptom that most women carry into their workdays. This article explores five distinct causes of perimenopause exhaustion and offers practical solutions for each.
In 2026, an international survey of more than 17,000 women across 158 countries highlighted a significant gap between expectation and reality. When asked which perimenopause symptoms they anticipated versus what they actually experienced, the answers were nearly opposites. While 71% expected hot flashes, the most frequent symptoms were fatigue and total physical and mental exhaustion, each reported by 83% of participants. Irritability, sleep disruptions, and mood changes followed closely behind.1
For decades, the clinical focus has remained on the physical symptoms. You might visit a doctor concerned about your energy and mental clarity, only to be questioned about hot flashes. This menopause exhaustion is often dismissed as a byproduct of a busy life, motherhood, or simply being a woman in her forties. However, it is biology.
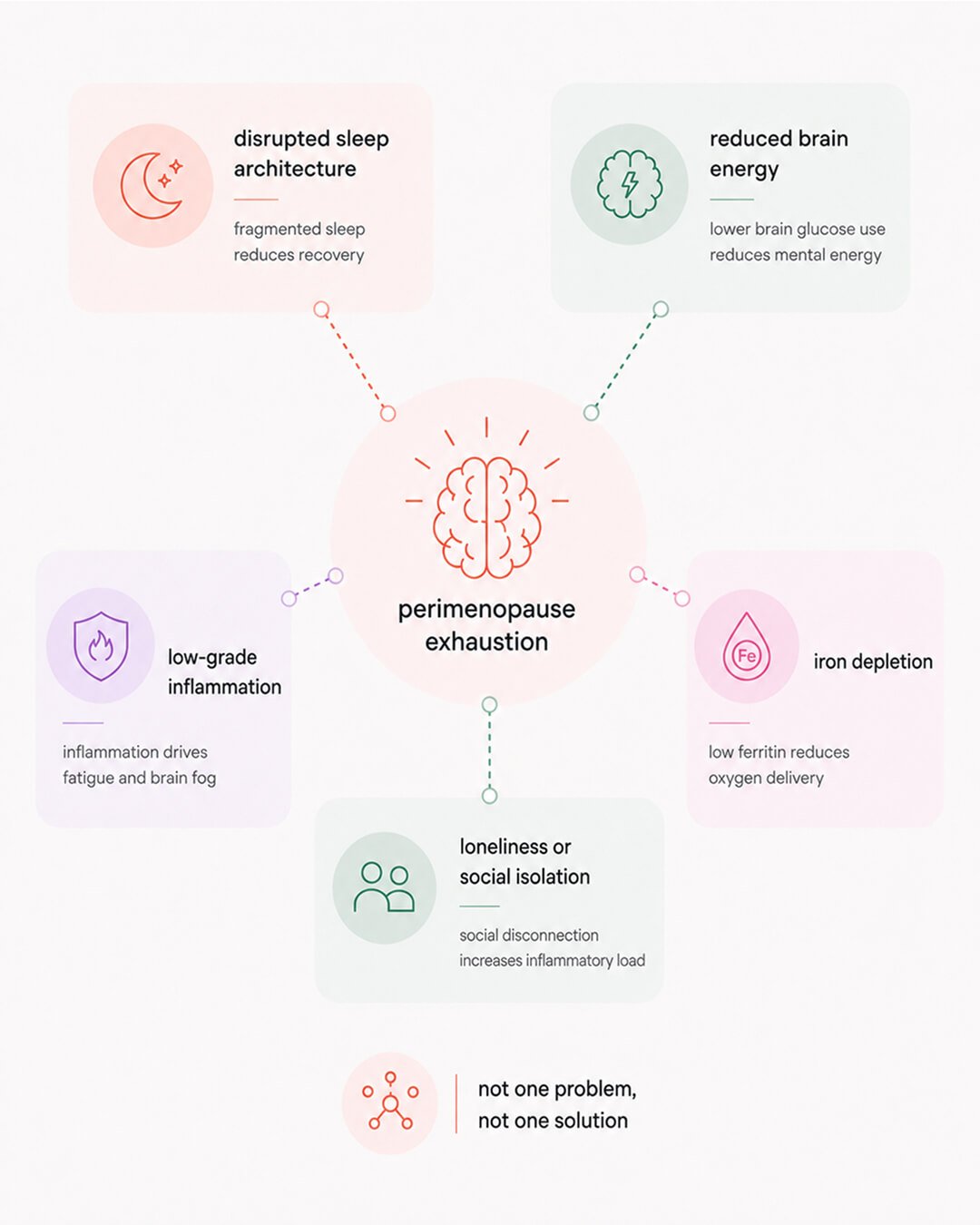
Addressing this requires looking at five specific biological drivers. Each has a different cause, a different solution, and a different timeline for improvement. Relying on a single intervention for all five is why many women feel as though nothing works.
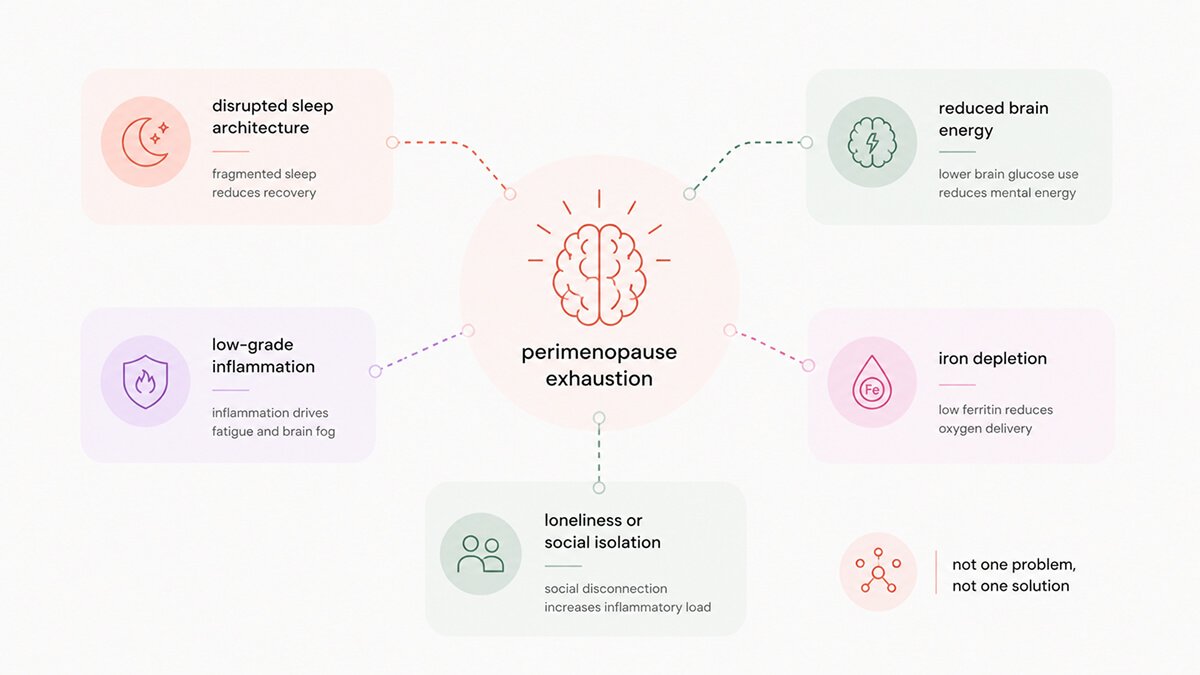
The first cause is sleep structure, rather than sleep duration. Each night, your brain moves through cycles of deep sleep for physical restoration and REM (rapid eye movement) sleep for emotional processing. These stages depend on stable hormones. During perimenopause, progesterone levels drop, leading to a decrease in a metabolite allopregnanolone. Allopregnanolone acts on the same brain receptors as prescription sleep medications. This substance naturally calms the brain; without it, the body loses its built-in sedative.2
Additionally, the temperature shifts that cause night sweats often wake you during the brain’s most critical repair windows. Even if you don’t remember waking up, your brain does. You may spend eight hours in bed but only experience the recovery of five.3
Finally, the brain’s master clock, the suprachiasmatic nucleus, relies on estrogen to stay in sync. As estrogen levels fluctuate and fall, this internal clock drifts. Your wake-up signals arrive at the wrong time, and your body loses the rhythm it has followed for decades.4
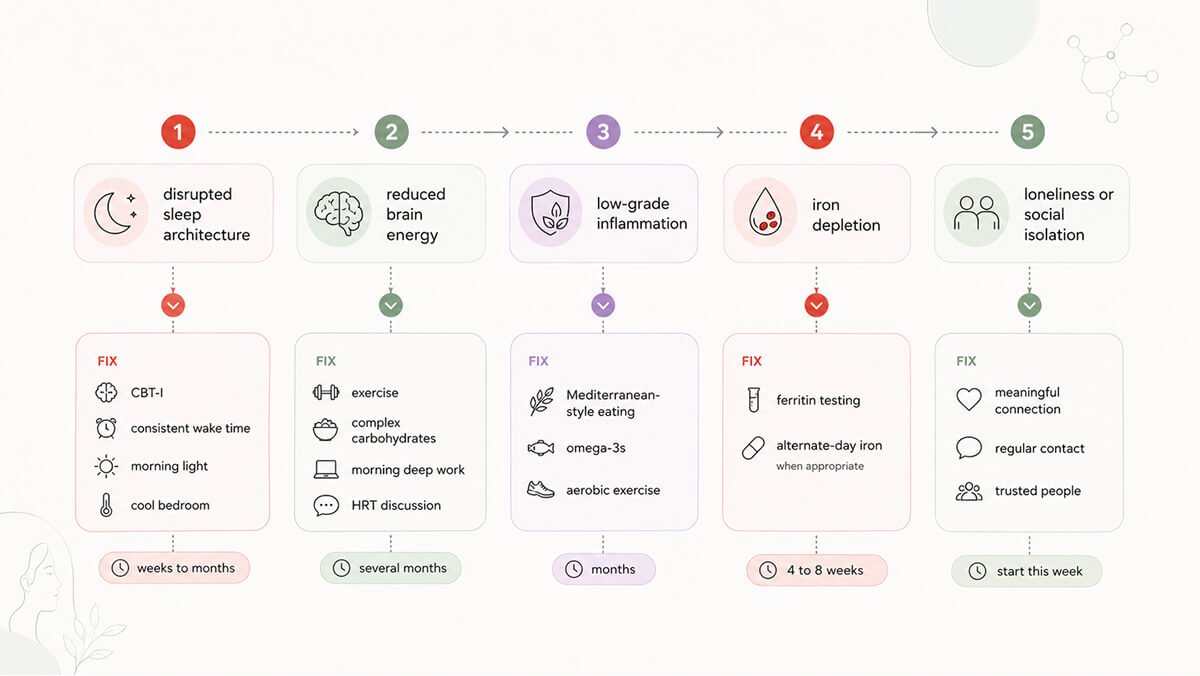
The most effective non-medication treatment for chronic sleep issues is cognitive behavioral therapy for insomnia (CBT-I), which retrains the brain’s response to bedtime.5 Beyond this, three habits are particularly effective. First, maintain a consistent wake-up time every day, including weekends, to anchor your internal clock. Second, get bright light in your eyes within the first hour of waking to signal a reset to your brain. Third, keep your bedroom slightly cooler than feels comfortable. Preventing temperature-driven wake-ups is essential for protecting the sleep cycles you need most.
While your brain represents only 2% of your body weight, it consumes 20% of the energy you eat. This energy is generated by mitochondria, the small power plants inside every neuron. Estrogen acts as a master regulator for these engines, controlling how neurons take in glucose and convert it into the fuel that powers your thoughts.6
When estrogen levels drop, brain energy production often drops with it. Scans show this clearly: a 2017 study of women aged 40 to 60 found that those in perimenopause had a significant reduction in brain glucose metabolism compared to premenopausal women.7 This decline was visible even before their final period. At a cellular level, their brains were struggling to produce enough energy for the same cognitive workload.
The daily experience of menopause exhaustion reflects this biological shift. You might have enough energy to lead a morning meeting but find your reserve empty by 2pm. Tasks that once felt effortless now require a deliberate, draining effort.
It isn’t only about glucose. Estrogen also supports the chemical messengers (neurotransmitters) that handle motivation, mood, and alertness: dopamine, serotonin, and norepinephrine. As estrogen declines, these signals can weaken. Your motivation might flatten, and things that used to feel rewarding can start to feel neutral. These aren’t psychological failings; perimenopause and menopause exhaustion are the neurochemistry of estrogen withdrawal.
Curious Fact. Imaging studies show that the shift in how the brain uses energy begins during the transition, not after it. Perimenopausal brains in their forties are already using less glucose than the brains of women just ten years younger.7
For women who are medically eligible, hormone replacement therapy (HRT) can help. The 2025 International Menopause Society guidelines confirm HRT as the most effective treatment for several menopause symptoms, with secondary benefits for sleep and mood.⁸ Whether HRT is right for you depends on your personal health history and should be a conversation with your doctor.
Beyond medication, exercise is a primary tool for brain energy that helps with menopause exhaustion. Strength and endurance training signal your cells to build more mitochondria, essentially creating more engines to power your brain.9 Opting for complex carbohydrates like legumes and vegetables instead of refined sugars can also prevent the blood-sugar crashes that make fatigue worse. Finally, scheduling your most demanding mental work for the morning isn’t just a productivity hack; it is a practical way to work within the energy reserves you actually have.
The third factor causing menopause exhaustion is inflammation – a piece of the puzzle that rarely gets mentioned.
Estrogen acts as a powerful anti-inflammatory agent for the brain. It keeps the brain’s immune cells, called microglia, in check and prevents inflammatory proteins from rising.10 When estrogen levels decline, those controls are lifted. The result is a persistent, low-grade inflammation. It isn’t enough to make you feel “sick” in the traditional sense, but it fundamentally changes your daily experience of menopause exhaustion.
This state triggers a specific set of symptoms that researchers have studied for decades. When inflammatory markers reach the brain, they produce what is known as “sickness behavior.” This includes fatigue, brain fog, slowed movement, and a desire to withdraw from social life.11 This matches the profile of perimenopause exhaustion. Inflammation isn’t just a side effect; it runs beneath the other symptoms and makes them feel more intense.
The shift in body composition that often starts during this time also plays a role. Visceral fat, the kind that surrounds your organs, is more than just stored energy. It is metabolically active tissue that releases inflammatory markers directly into your system.12 The increase in this specific type of fat, combined with the loss of estrogen, creates a feedback loop that keeps your energy levels low.
A Mediterranean-style diet focused on fish, olive oil, vegetables, and whole grains is one of the most effective ways to lower chronic inflammation.13 High-quality Omega-3 supplements, specifically a mix of EPA and DHA, can also help reduce inflammatory markers.14 Finally, regular aerobic exercise is a reliable tool for cooling this internal fire. Activities that get you breathing harder but still allow you to speak in short sentences can lower inflammatory signals within just a few weeks of consistent effort.15
The fourth cause is often missed in clinical visits because it has nothing to do with what doctors usually look for during perimenopause.
Roughly one in three women experience abnormal bleeding during the menopause transition, which can mean heavier periods, longer periods, or unpredictable timing.16 While this is common, it has real consequences especially for perimenopause exhaustion. Blood loss means iron loss. Your red blood cells rely on iron to carry oxygen to every tissue in your body, including your brain. Research shows that iron deficiency, even without full-blown anemia, is consistently linked to fatigue, brain fog, and worsened mental health.17 From the inside, iron-driven fatigue feels exactly like hormone-driven menopause fatigue.
A 2025 analysis from the Study of Women’s Health Across the Nation (SWAN) confirmed this connection directly. Researchers tracked over 2,300 women and found that those who had three or more heavy periods in a six-month window were 62% more likely to report feeling tired. This remained true even when factoring out sleep problems, stress, and other known variables.18 The bleeding itself was draining their energy.
The key clinical detail here is the difference between two common blood tests. A standard hemoglobin test measures the iron currently circulating in your red blood cells. It can look perfectly normal even as your body’s iron reserves drop to zero. A ferritin test measures the iron you have in storage. If you have dealt with heavy periods for a year and your doctor told you your blood work was fine, they likely did not test your ferritin.
Ask your doctor specifically for a ferritin test. If your levels are low, iron supplementation can change how you feel faster than any other strategy mentioned here. Current evidence points to moderate doses of oral iron, like ferrous bisglycinate, taken in the morning. Taking it every other day is actually more effective than taking it daily. Alternate-day dosing improves absorption by working around hepcidin, a hormone that temporarily blocks iron uptake after a dose.19 Most women notice a real difference of menopause exhaustion within four to eight weeks, making this the fastest timeline of anything on this list.
The fifth cause of menopause exhaustion is often dismissed as a lifestyle issue, but the science says otherwise.
A 2026 study of 903 perimenopausal women found that loneliness, the feeling of being disconnected, and social isolation, the actual lack of contact, both independently drive cognitive decline. Women who experienced both at moderate to severe levels had the highest risk of severe cognitive symptoms.20
The biology behind this aligns with what we already know about the transition. Loneliness is consistently tied to higher markers of inflammation, specifically a protein called IL-6. Social isolation also triggers chronic systemic inflammation on its own.21 Both of these fuel the exact same inflammatory fire that dropping estrogen levels have already started. Furthermore, isolation strips away the cognitive stimulation that keeps your brain’s networks sharp. Perimenopause already places stress on your brain’s adaptability and regulation systems; loneliness pushes them further.
The menopause transition often happens exactly when your social structures begin to shift. Children move out, friendships change due to career or life logistics, and aging parents suddenly require more care. You might be the person holding everything together for everyone else. When you are completely exhausted, the natural response is to cancel dinner, skip coffee, and retreat to a quiet room. Most of us have done some version of this. As a short-term strategy to survive a hard week, it is fine. But when it becomes a pattern, it makes the menopause exhaustion worse.
The answer is not networking, nor is it superficial advice to simply “be more social.” The interactions that actually improve your biology and ease menopause exhaustion are the ones with substance. It means having one good conversation with someone who really knows you, maintaining a weekly call with a close friend, or engaging genuinely with a colleague. You can skip the events that drain your energy. The goal is not a high volume of contact. The goal is a meaningful connection that reactivates the biological systems you need most.

When you look at a list of causes like this, it is natural to want to find the single reason that explains everything. But perimenopause exhaustion is rarely just one issue. It is usually a combination of factors, each contributing to the fatigue and each requiring its own specific response.
The timelines for recovery are also different. If your iron is low, supplementation can change how you feel in four to eight weeks. Sleep structure takes weeks or a few months to improve. Inflammation cools down gradually over many months of consistent food and exercise changes. Hormone therapy, if you and your doctor decide it is right for you, takes several months to reach full effect. The social piece is something you can start this week.
You do not have to tackle all five at once. The goal is to figure out which issue is doing the most damage right now and start there. For most women, the smartest first step is a blood test to check ferritin. Next is sleep. After that, address the remaining areas in the order that makes the most sense for your life and your schedule.
Most importantly, this is not a personal failing. You are not weak, you are not lazy, and you are not aging faster than everyone else. You are simply operating a body with a changed hormonal baseline and a brain that was built to run on a level of estrogen that is no longer there.
Perimenopause exhaustion is not a single problem with a single solution. It is five biological changes happening at the exact same time in midlife: fragmented sleep, declining brain energy, chronic inflammation, iron depletion, and a disrupted social biology. When a woman is simply told to manage her stress and sleep more, she is only being treated for a fraction of the problem.
The practical path forward is to figure out which of these causes are the loudest in your own life, address them systematically, and understand that recovery happens on different timelines. None of it is personal.
Dr. Jura Lasas
1.
Hedges M.S. et al. Global perspectives on perimenopause: a digital survey of knowledge and symptoms using the Flo application (2026). https://doi.org/10.1097/GME.0000000000002730
2.
Standeven L.R. et al. Allopregnanolone and reproductive psychiatry: an overview (2022). https://doi.org/10.1080/09540261.2018.1553775
3.
Joffe H. et al. Evaluation and management of sleep disturbance during the menopause transition (2010). https://doi.org/10.1055/s-0030-1262900
4.
Hatcher K.M. et al. Estrogens and the circadian system (2022). https://doi.org/10.1016/j.semcdb.2021.04.010
5.
Pak D. et al. Effects of cognitive behavioral therapy on sleep quality and insomnia severity index in women with menopausal insomnia: a systematic review and meta-analysis (2025). https://doi.org/10.4069/whn.2025.09.07
6.
Yao J., Brinton RD. Estrogen regulation of mitochondrial bioenergetics: implications for prevention of Alzheimer’s disease (2012). https://doi.org/10.1016/B978-0-12-394816-8.00010-6
7.
Mosconi L. et al. Perimenopause and emergence of an Alzheimer’s bioenergetic phenotype in brain and periphery (2017). https://doi.org/10.1371/journal.pone.0185926
8.
International Menopause Society. IMS recommendations and key messages on women’s midlife health and menopause (2025). https://doi.org/10.1080/13697137.2025.2585487
9.
Granata C. et al. Training-induced changes in mitochondrial content and respiratory function in human skeletal muscle (2018). https://doi.org/10.1007/s40279-018-0936-y
10.
Vegeto E. et al. The role of sex and sex hormones in neurodegenerative diseases (2020). https://doi.org/10.1210/endrev/bnz005
11.
Dantzer R. et al. From inflammation to sickness and depression: when the immune system subjugates the brain (2008). https://doi.org/10.1038/nrn2297
12.
Kawai T. et al. Adipose tissue inflammation and metabolic dysfunction in obesity (2021). https://doi.org/10.1152/ajpcell.00379.2020
13.
Schwingshackl L., Hoffmann G. Mediterranean dietary pattern, inflammation and endothelial function: a systematic review and meta-analysis of intervention trials (2014). https://doi.org/10.1016/j.numecd.2014.03.003
14.
Li K. et al. Effect of marine-derived n-3 polyunsaturated fatty acids on C-reactive protein, interleukin 6 and tumor necrosis factor α: a meta-analysis (2014). https://doi.org/10.1371/journal.pone.0088103
15.
Zheng, G., et al. Effect of aerobic exercise on inflammatory markers in healthy middle-aged and older adults: a systematic review and meta-analysis of randomized controlled trials (2019). https://doi.org/10.3389/fnagi.2019.00098
16.
Paramsothy P. et al. Bleeding patterns during the menopausal transition in the multi-ethnic Study of Women’s Health Across the Nation (SWAN): a prospective cohort study (2014). https://doi.org/10.1111/1471-0528.12768
17.
Greig, A.J., et al. Iron deficiency, cognition, mental health and fatigue in women of childbearing age: a systematic review (2013). https://doi.org/10.1017/jns.2013.7
18.
Harlow S.D., et al. Abnormal uterine bleeding is associated with fatigue during the menopause transition (2025). https://doi.org/10.1097/GME.0000000000002525
19.
Stoffel N.U., et al. Iron absorption from oral iron supplements given on consecutive versus alternate days and as single morning doses versus twice-daily split dosing in iron-depleted women: two open-label, randomised controlled trials (2017). https://doi.org/10.1016/S2352-3026(17)30182-5
20.
Lin X., et al. Independent and joint associations of loneliness and social isolation with subjective cognitive decline in perimenopausal women (2026). https://doi.org/10.1097/GME.0000000000002763
21.
Smith K.J., et al. The association between loneliness, social isolation and inflammation: a systematic review and meta-analysis (2020). https://doi.org/10.1016/j.neubiorev.2020.02.002

Mood & Energy Solutions
Fatigue Causes & Types
Fatigue Causes & Types

Workplace Strategies

Menopause at Work

Brain Fog at Work

Brain Fog at Work

Is This Perimenopause?

Is This Perimenopause?

Nutrition & Supplements

Workplace Strategies

Menopause Science

Menopause Science

Brain Fog Solutions
We use cookies and similar technologies to ensure the proper functioning of our website, personalize content, provide social media features, and analyze traffic. By clicking “I Agree”, you consent to the use of these technologies.
No results





