22 June 2026
Menopause Nervous System Support: What Perimenopause Guidelines Still Miss

Reading time 16 min.

Reading time 16 min.
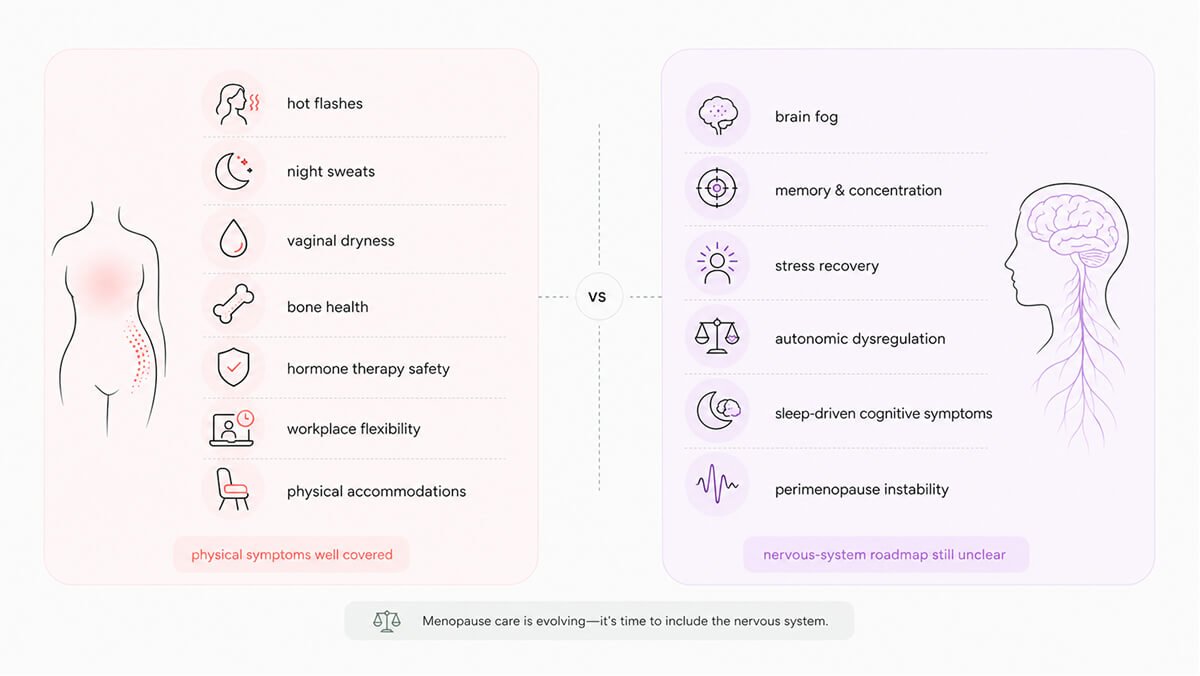
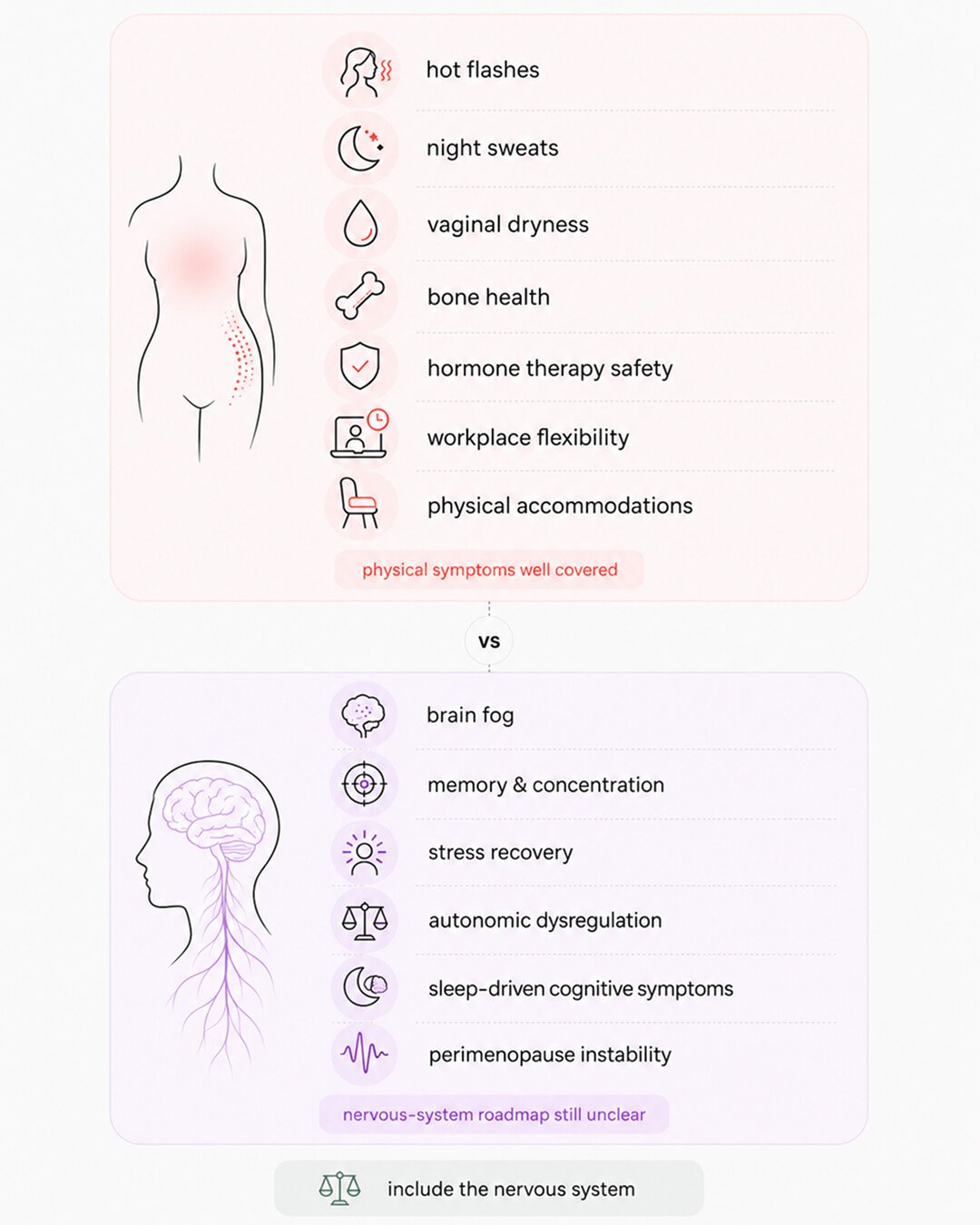
Most menopause treatment plans are built around what a doctor can see and measure. Hot flashes, night sweats, painful sex, bone density loss. The major Western guidelines explain how to manage each one well, with hormone therapy as the first option and a clear set of safety rules around it. None of these are the symptoms that make a senior professional woman start to question her competence in a meeting. Those symptoms belong to the menopause nervous system: the cognitive, mood, sleep, and autonomic effects of estrogen change in the brain. Despite their impact, major medical guidelines rarely address the menopause nervous system in a structured way. The research on how perimenopause affects the brain has been clear for years, yet this information is rarely shared with clinicians or patients. Consequently, most women are left without a roadmap for the very symptoms that affect their professional and mental lives the most.
Standard Western medical guidelines are in broad agreement: Hormone Replacement Therapy (HRT) is the most effective treatment for hot flashes, night sweats, vaginal dryness, and bone loss¹. This position is held by major organizations, including NAMS (US), NICE (UK), the International Menopause Society, and the latest 2025 European guidelines.
Reflecting this consensus, the FDA recently removed decades-old black box warnings from hormone therapy products. The evidence shows that for women under 60 or within 10 years of menopause, the benefits of managing hot flashes and protecting bone health outweigh the risks.1
However, timing is critical. Starting hormone therapy early carries a favorable profile, but starting it more than 10 years after menopause (or after age 60) increases the risks of heart disease, stroke, and dementia.¹ It is also important to note what HRT is officially approved for: physical symptoms and bone health. It is not currently approved as a standalone treatment for cognitive issues, mood disorders, or sleep problems.
For women with a uterus, a combination of estrogen and progestogen is required to protect the uterine lining. For those who cannot use hormones, due to a history of breast cancer, blood clots, or liver disease, guidelines offer several alternatives:
Lifestyle changes, such as exercise, maintaining a healthy weight, and limiting alcohol, are recommended by every major guideline as a supporting layer, though they are rarely positioned as a primary treatment for severe symptoms.
In a clinical setting, a standard plan typically starts with a symptom assessment, followed by hormone therapy. Doctors generally prefer transdermal estradiol (patches or gels) to lower blood clot risk and micronized progesterone to lower breast cancer risk. While this approach is thorough, it is designed to treat what can be counted or measured: the frequency of hot flashes, bone density scores, and heart disease risk. The more complex perimenopause nervous system remains largely outside this traditional measurement frame.
While brain science is still catching up, workplace guidelines have evolved rapidly. Major organizations like the European Menopause and Andropause Society (EMAS) and The Menopause Society in the US have recently published workplace standards.2,3 The UK offers the strongest legal protections, where severe symptoms can be classified as a disability, legally requiring employers to provide “reasonable adjustments.”
Current global guidelines recommend that employers take three main steps:
Manager training is the support most requested by women. Organizations now recommend training managers on how to have sensitive conversations and how to understand the legal risks of discrimination. Many companies are also appointing “menopause champions” – peer contacts who normalize the topic and help colleagues navigate HR or healthcare options. In the US, a key recommendation is for employers to ensure their health insurance plans specifically cover menopause specialists and treatments.3
For women managing their own care, the guidance is consistent:
While these workplace protections, like fans and flexible hours, are valuable, they often miss the core issue for women in leadership. According to the EMAS consensus, most women in perimenopause cite difficulties with concentration, memory, and planning as their biggest professional hurdle.². Unfortunately, current guidelines rarely offer specific solutions for these cognitive symptoms beyond general lifestyle advice. For now, managing the “cognitive nervous system” during perimenopause remains a challenge women are largely expected to handle on their own.
In March 2026, the International Federation of Gynecology and Obstetrics (FIGO) published a landmark set of recommendations for mental health during menopause.4 This global effort, involving experts from eight countries, addressed 13 key questions regarding anxiety, depression, and mood swings. A vast majority of these experts gave strong recommendations for new standards of care.
The FIGO guidelines represent a major shift in several ways:
This position is a breakthrough because it validates that perimenopausal anxiety and depression are rooted in biology and may require hormonal treatment.
However, even these updated guidelines do not address the specific cognitive symptoms that impact women in high-level professional roles. While FIGO covers mood and mental health, it does not provide a roadmap for the brain fog symptoms, such as losing your train of thought, struggling to recall names, or the increased mental effort required to juggle complex tasks. The cognitive side of the perimenopause nervous system remains the missing piece in formal medical guidance.
Current medical guidelines still have significant blind spots when it comes to the perimenopause nervous system. While physical symptoms are well-documented, the cognitive and neurological shifts women experience remain largely unaddressed.
Here are the four primary gaps in current medical guidance:
No major Western guideline includes a formal protocol for brain health or cognitive assessment during perimenopause. While the International Menopause Society released a “brain fog” white paper in 2022 to help doctors talk to patients, it isn’t a clinical treatment plan.⁵ There are currently no validated screening tools or decision trees to help doctors determine when cognitive symptoms require intervention.
The symptoms themselves are well-documented; the long-running SWAN study has shown that women’s performance on memory and processing speed tests changes measurably during the transition.⁶ Furthermore, while early hormone therapy may help, starting it too late does not offer the same cognitive protection.
The nervous system’s stress circuit (the HPA axis) becomes much more sensitive as estrogen fluctuates. This leads to autonomic dysregulation, which feels like a lower tolerance for stress, difficulty recovering from a hard day, and persistent fatigue. Despite this, major guidelines (such as NAMS, NICE, or the NHS) do not list these autonomic effects as specific targets for treatment. The closest recognition we have is FIGO’s 2026 acknowledgment that mood is rooted in biology.
While every guideline mentions sleep hygiene, none treat sleep as the primary driver of brain function. Sleep is when the brain clears out waste and solidifies memories. During perimenopause, broken sleep is a leading cause of “brain fog” and slow word retrieval the next day, yet it isn’t prioritized as a key way to protect cognitive health.
Most research and guidelines focus on postmenopause. However, perimenopause is biologically different; instead of a steady decline, estrogen levels are volatile, swinging through high peaks and deep troughs. The brain is reacting to this instability, yet medical frameworks still treat perimenopause as a side issue rather than a unique phase that requires its own specific care.
A Curious Fact: Despite exercise being the most commonly recommended intervention for brain health, as of 2025, there has not been a single published randomized clinical trial specifically testing the effects of exercise on the cognitive function of perimenopausal women. The first trial designed to bridge this gap was only recently registered.
While specific research on perimenopause is still catching up, the core principles of healthy brain aging are well-established. We know what protects the brain throughout life, and there is every reason to believe these same levers are vital during the menopausal transition.
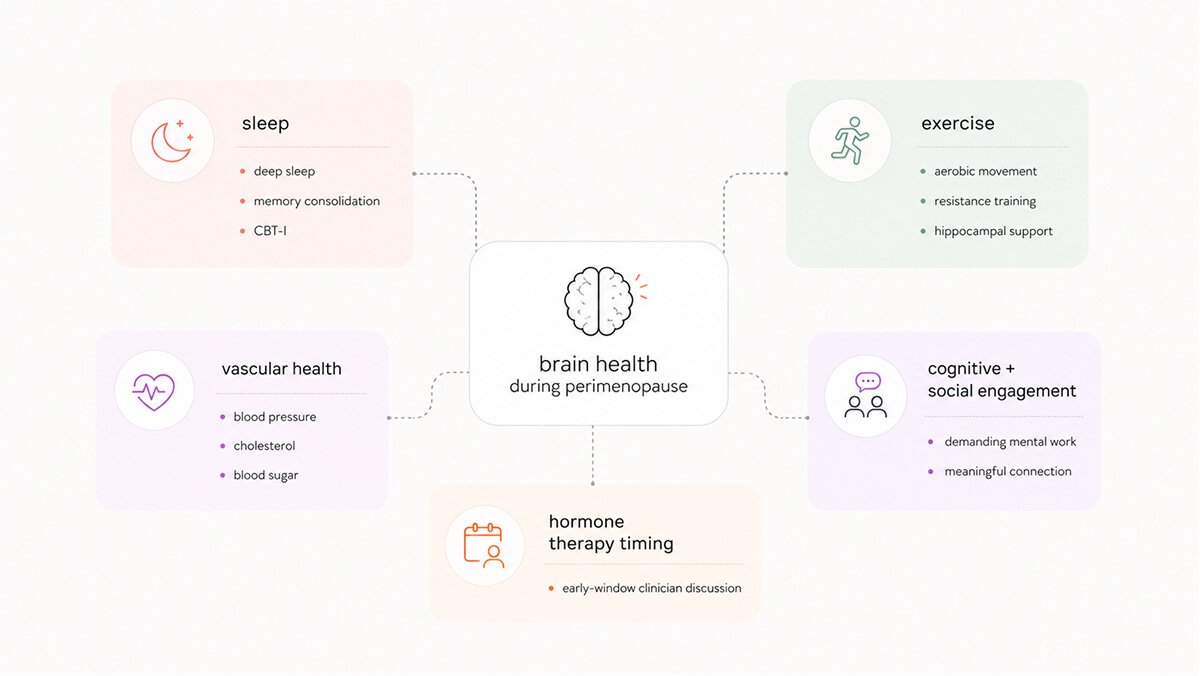
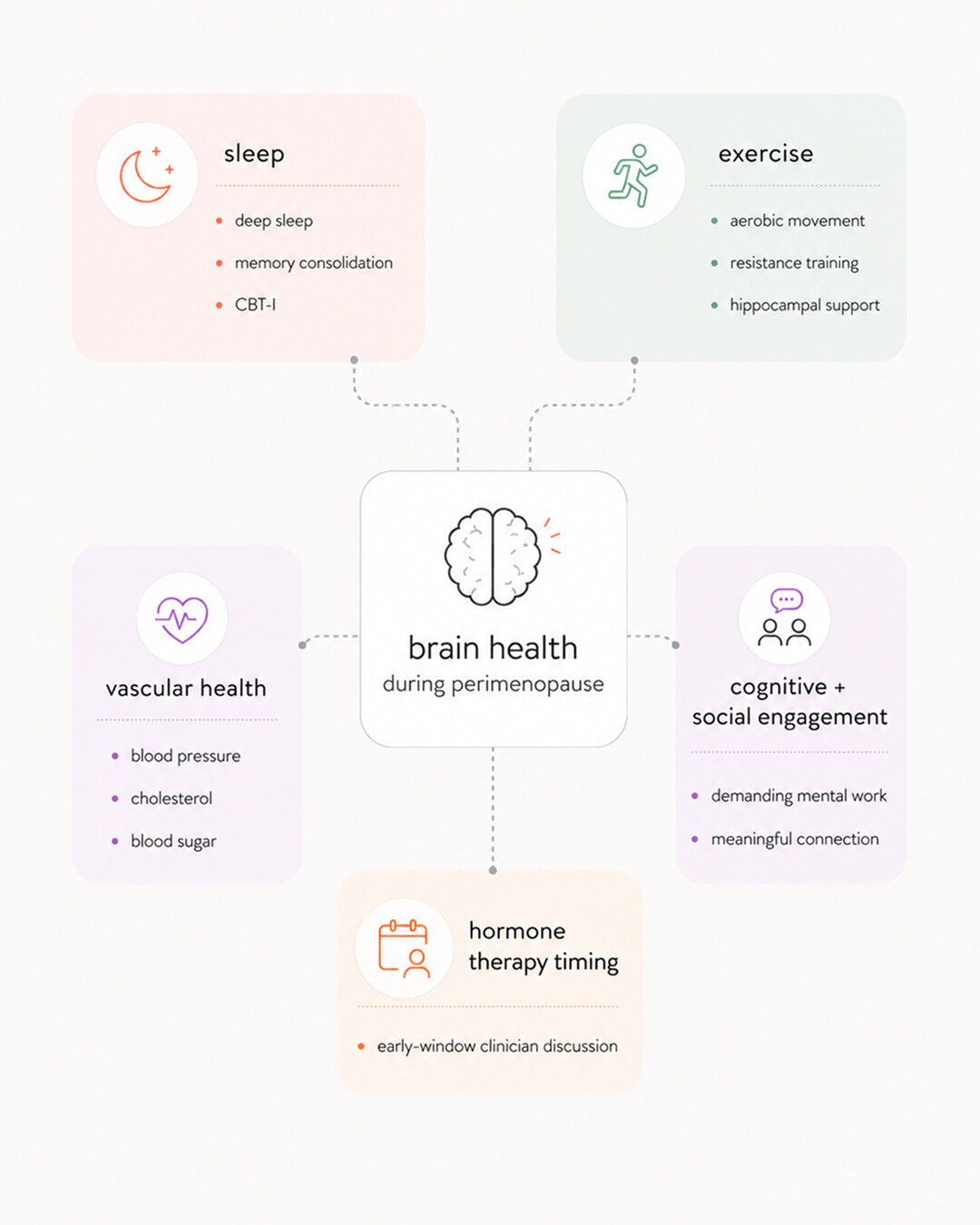
Based on large-scale dementia prevention studies, here are the five primary ways to protect your brain health:
Sleep is your most important cognitive tool. During deep sleep, your brain clears out metabolic waste, including proteins linked to Alzheimer’s, and saves the day’s experiences into long-term memory. Because perimenopause often disrupts sleep, the mental cost (slower thinking and poor memory) is immediate.
Cognitive Behavioral Therapy for Insomnia (CBT-I) has the strongest evidence for treating chronic sleep issues during this transition, yet it remains one of the most underused treatments.
Physical activity is one of the top modifiable risk factors for preventing dementia. Aerobic exercise has been shown to physically increase the size of the memory center (hippocampus), while resistance training boosts mental performance. If a specific exercise protects a 60-year-old brain, it is almost certainly protecting a 45-year-old brain facing hormonal volatility.
Brain health is inseparable from heart health. High blood pressure, high cholesterol, and elevated blood sugar all damage the blood vessels that feed the brain. As estrogen’s protective effect on your arteries fades during perimenopause, managing these vascular factors becomes a critical part of your brain-protection strategy.
Staying mentally challenged and socially connected acts as a shield against decline. For women in senior professional roles, this lever is already at work. While demanding, complex problem-solving and constant decision-making at work provide the exact kind of “cognitive engagement” that protects the aging brain.
While hormone replacement therapy (HRT) is not officially approved to treat brain fog, timing is everything. Data suggests a critical window: estrogen may benefit brain function when started early in the transition, whereas starting it much later (after age 60) can actually increase risks. Any decision about HRT is, indirectly, a decision about your brain’s aging trajectory.
We have the science to build a perimenopause nervous system protocol based on sleep, movement, vascular health, mental engagement, and hormonal timing. Even if a formal medical checklist doesn’t exist yet, these five levers are the best “insurance” available for your brain.
The menopause nervous system represents the area where senior professional women feel their careers are most vulnerable and where the gap between scientific research and medical guidance is widest. Although perimenopause-specific clinical trials are still catching up, the broader science of brain aging already provides a clear and actionable roadmap.
To navigate this transition effectively, the most critical steps are to aggressively protect sleep, maintain a daily exercise routine, prioritize heart health, and continue engaging in demanding cognitive work.Most importantly, women should have proactive conversations with knowledgeable clinicians about the timing of hormone therapy while they are still within the early window of opportunity. Moving from a mindset of body maintenance to one of brain insurance allows women to protect their cognitive performance and professional confidence even as their hormones fluctuate.
Dr. Jura Lasas
1.
The 2022 Hormone Therapy Position Statement of The North American Menopause Society (2022). https://doi.org/10.1097/GME.0000000000002028
2.
Rees, M. et al. Global consensus recommendations on menopause in the workplace: A European Menopause and Andropause Society (EMAS) position statement (2021). https://doi.org/10.1016/j.maturitas.2021.06.006
3.
The Menopause Society. Menopause and the workplace: consensus recommendations from The Menopause Society (2024). https://doi.org/10.1097/GME.0000000000002415
4.
Khadilkar, S. et al. FIGO best practice recommendations for the mental health of women at menopausal age (2026). https://doi.org/10.1002/ijgo.70943
5.
Maki, P.M. and Jaff, N.G. Brain fog in menopause: a health-care professional’s guide for decision-making and counseling on cognition (2022). https://doi.org/10.1080/13697137.2022.2122792
6.
Greendale, G.A., Derby, C.A. and Maki, P.M. Perimenopause and cognition (2011). https://doi.org/10.1016/j.ogc.2011.05.007
7.
Livingston, G. et al. Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission (2024). https://doi.org/10.1016/S0140-6736(24)01296-0
8.
Mosconi, L. et al. In vivo brain estrogen receptor density by neuroendocrine aging and relationships with cognition and symptomatology (2024). https://doi.org/10.1038/s41598-024-62820-7
Mood & Energy Solutions

Fatigue Causes & Types
Fatigue Causes & Types

Workplace Strategies

Menopause at Work

Brain Fog at Work

Brain Fog at Work

Is This Perimenopause?

Is This Perimenopause?

Nutrition & Supplements

Workplace Strategies

Menopause Science

Menopause Science

Brain Fog Solutions
We use cookies and similar technologies to ensure the proper functioning of our website, personalize content, provide social media features, and analyze traffic. By clicking “I Agree”, you consent to the use of these technologies.
No results





