22 June 2026
Menopause Brain Fog: Causes, Brain Science & What Actually Helps

Reading time 13 min.

Reading time 13 min.
You’re introducing your manager Sarah to a client you’ve worked with for three years. You’ve said her name a hundred times. And you just can’t remember her name is Sarah. You keep talking and gesture toward her, buy yourself two seconds. Finally, you remember! But the moment and the quiet panic underneath stay with you for the rest of the day.
This event has a name, “brain fog”, a mechanism, and research behind it. Between 50 and 75% of women experience cognitive changes during perimenopause and more when you count the women who notice but say nothing. It is not a mood, not tiredness. Brain fog is a specific, documented change in brain biology. This experience is one of the most common signs of menopause brain fog, even in high-functioning women.
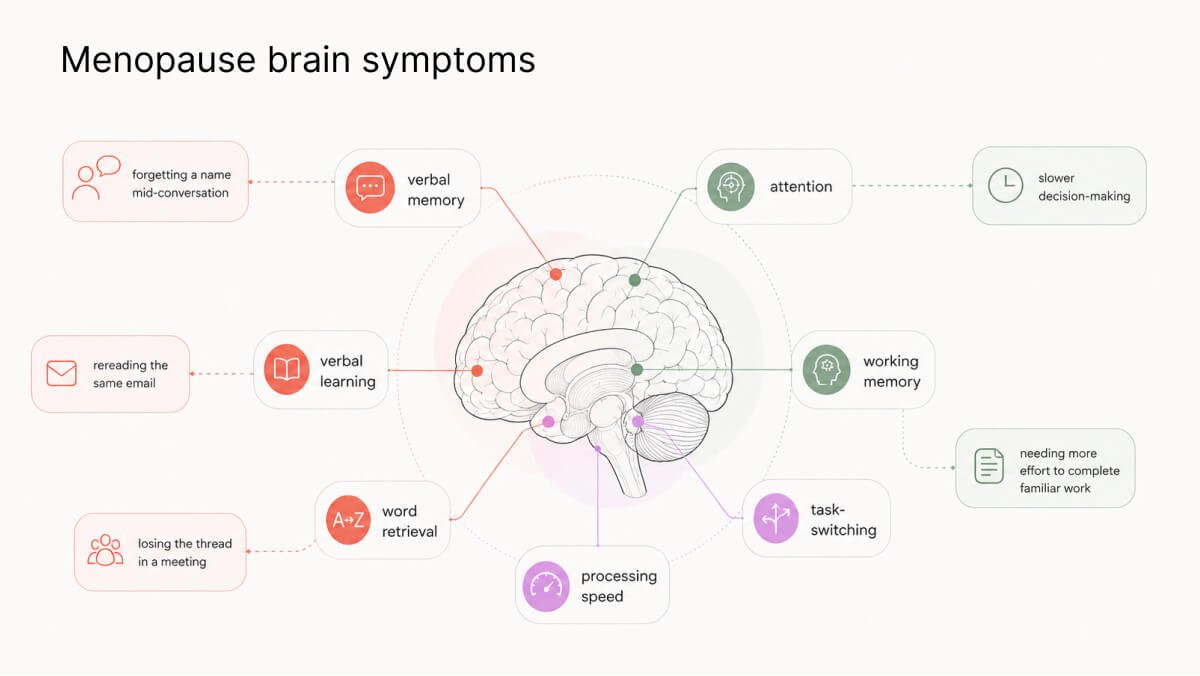
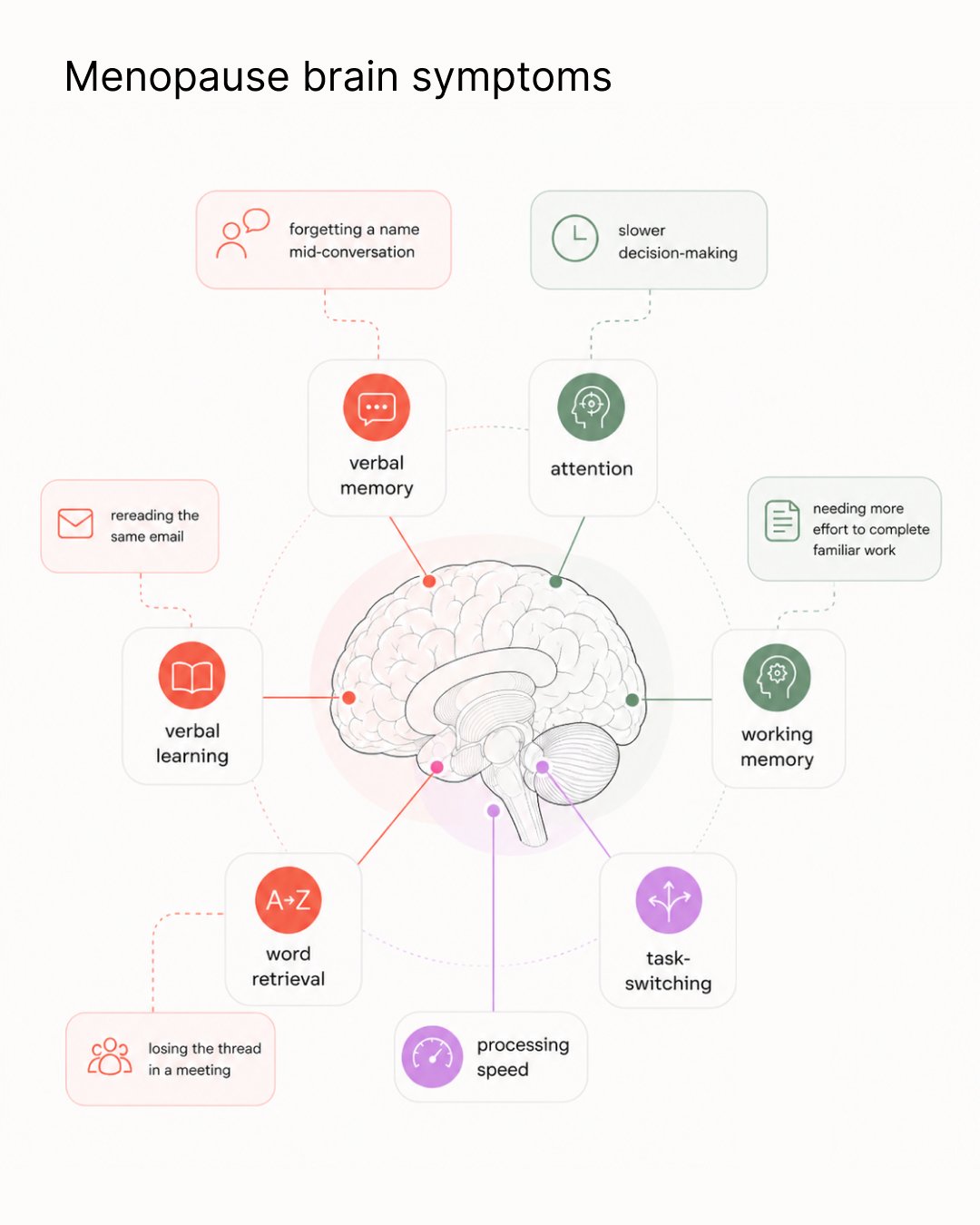
Menopause brain fog is not one symptom but rather a collection of symptoms.
Your verbal memory and verbal learning are affected the most. This is what governs your ability to take in new information under pressure, pull up a name or word mid-conversation, and hold the thread of a complex argument for an entire meeting. Data from the Study of Women’s Health Across the Nation (SWAN) and the Rochester Investigation of Cognition Across Menopause (RICAM) show the same pattern: verbal memory scores that normally improve with repeated testing in midlife simply stop improving during perimenopause.3
Processing speed is the next one to be affected. In SWAN, psychomotor speed declined roughly 4.9% over 10 years during the transition.3 More recent data shows declines in attention and working memory as well. Executive function, encompassing decision-making, cognitive flexibility, and task-switching, presents the most ambiguous evidence, primarily because conventional cognitive assessments were tailored for older adults with clinical impairments rather than high-functioning women in their 40s who are aware of the disparity between their previous behaviors and the current effort required.3
If you’ve googled “brain fog” wondering if it’s real and come away more confused than when you started, that’s not your fault. The research looks contradictory until you understand what story the science tells. Studies that carefully define what “perimenopause” actually means find a clear, consistent cognitive effect. Studies that don’t use a precise definition for perimenopause find nothing. The biology is consistent and the brain fog is a real neurocognitive phenomenon. A 2025 meta-analysis of nearly 10,000 women confirmed it.1
Not every woman experiences the same cognitive changes. Research from RICAM followed 85 perimenopausal women across 400 visits and identified four distinct cognitive patterns:
About 23% had weaknesses in verbal memory specifically. And that group had one thing in common that the others didn’t: more sleep disturbance and less hormonal variability. The other 77% were in normal or above-normal territory for at least one domain. Most women going through perimenopause do not develop cognitive impairment. A significant minority do, and sleep is one of the clearest distinguishing factors.2
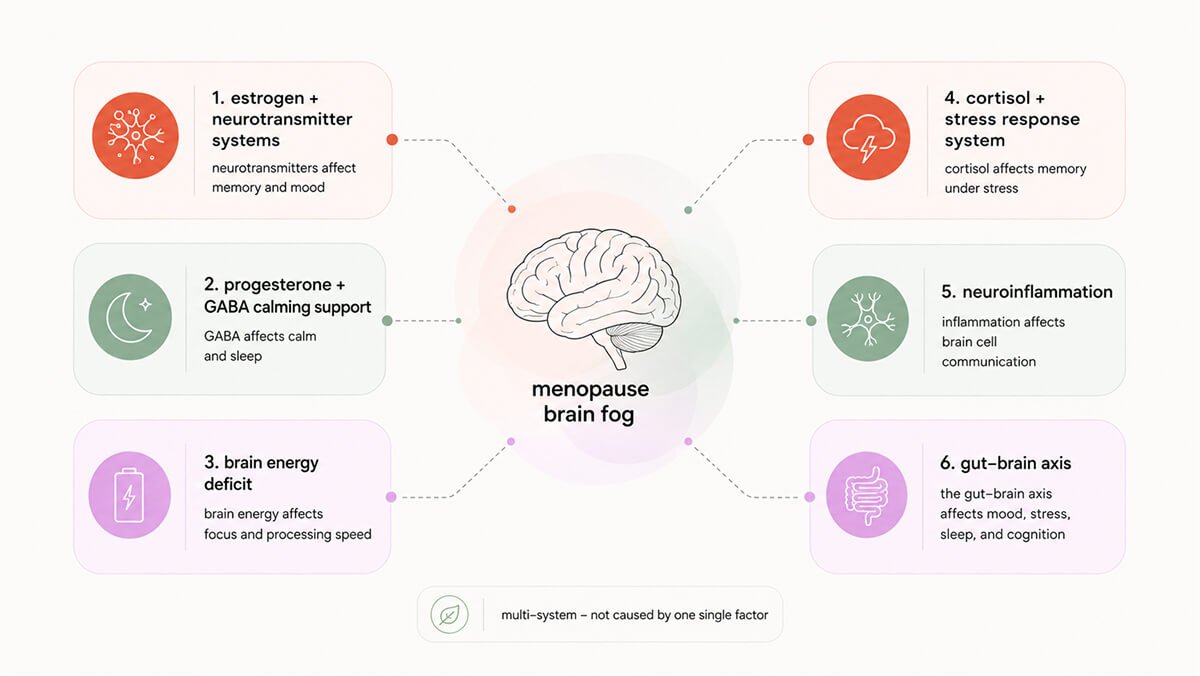
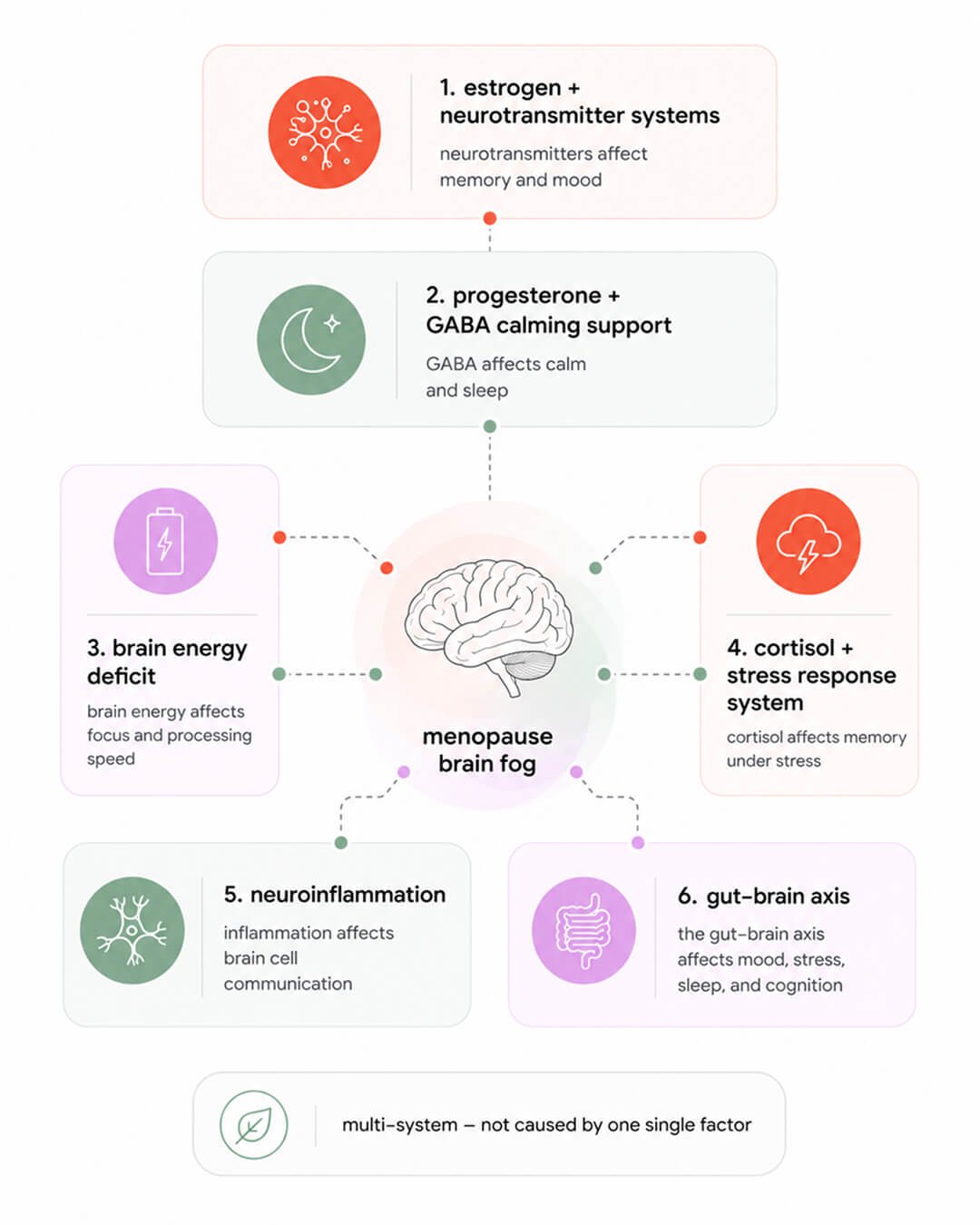
I identified six mechanisms that drive perimenopause brain fog.
Estrogen actively maintains the chemical infrastructure your cognition runs on. It does this through three major neurotransmitter systems simultaneously.
Estrogen also supports something called BDNF (brain-derived neurotrophic factor). Think of it as fertilizer for brain cells. It keeps neurons growing, connecting, and forming new memories. Estrogen levels affect BDNF levels as well. We can use exercise to help increase BDNF. However, when you look across multiple studies it depends on what kind of exercise you’re doing, how much of it, your baseline health, and even how BDNF is measured in the study. One small study in older adults (n=30) showed intriguing evidence that combining resistance training with simultaneous cognitive challenge increases BDNF by 53% when compared to the starting BDNF levels.12
Progesterone’s role in menopause brain fog is separate from estrogen’s, and it tends to get far less attention than it deserves. In the brain, progesterone is converted into allopregnanolone, which strongly activates GABA receptors. GABA is your brain’s main calming system. It helps quiet down background noise, supports sleep, and keeps your focus from getting pulled in every direction. When progesterone levels go down, your calming system becomes less stable.
When progesterone declines, neurons become more excitable. The brain becomes harder to quiet and anxiety increases. Sleep architecture changes, specifically the slow-wave stages are disrupted, which matters enormously for memory. Slow-wave sleep enables the hippocampus to transfer what you learned during the day into long-term storage. This mechanism means that even women without subjective insomnia may have compromised memory consolidation, simply from declining progesterone.
Think of the brain as a city running on electricity. Estrogen has been managing the power grid. When estrogen declines, the grid becomes unreliable. The regions most affected are those responsible for memory and executive function, and what they experience is a state of intermittent energy undersupply. The technical term is cerebral glucose hypometabolism.
In animal studies, overall brain glucose use drops by about 15%, and this comes with signs that mitochondria are not working as well and that oxidative stress is increasing. In humans, brain scans show a similar pattern. As women move through late perimenopause and into postmenopause, certain brain regions start using less glucose, especially areas linked to memory like the hippocampus and posterior cingulate. Under normal conditions, estrogen helps brain cells take in glucose, process it, and turn it into energy. When estrogen declines, that system becomes less stable. This is also reflected in the body more broadly, with increased insulin resistance, changes in how glucose is handled, and shifts in metabolic hormones.4
Perimenopause increases the risk of developing insulin resistance, which can put extra strain on the brain’s energy system. Neurons are already working less efficiently because of changes in estrogen and mitochondrial function. Now they also have a harder time getting glucose into the cell because of disrupted insulin signaling. It becomes a double hit to the same system. A 2025 longitudinal analysis found insulin sensitivity was significantly associated with slower cognitive decline specifically in women, with effects on both episodic memory and executive function.7 Insulin resistance is not something that happens to every woman during perimenopause. In women who develop blood sugar problems, this significantly amplifies what’s already happening. Which is why metabolic health during perimenopause should be seen as a brain concern, not just a metabolic one.
Curious Fact: The brain does not slow down during perimenopause. If anything, it works harder. Studies using phosphorus MRS show that perimenopausal women use more ATP, the brain’s energy currency, in frontal regions compared to men of the same age. The brain is spending more energy to produce the same level of focus, thinking, and output. That extra effort is a form of compensation. It helps maintain performance for a while, but it comes at a cost. How long that compensation can be sustained depends on several things, including genetics, cardiovascular health, and how well other systems like metabolism and sleep are functioning.5
Estrogen interacts directly with your slow stress system – the HPA axis, the brain-body pathway that controls cortisol. Signals start in the hypothalamus, move to the pituitary, and then to the adrenal glands, which release cortisol. Estrogen can change how strongly each step responds and how effectively the system shuts itself off after a stressor. Estrogen helps “tune” how sensitive your brain and body are to stress signals. You can think of it like adjusting the volume knob on your stress response. But the simple story that lower estrogen automatically means higher cortisol and a constantly overactive stress system doesn’t fully hold up in human studies.
What we actually see is more nuanced. Estrogen can change how strongly you react to stress and how quickly you recover, but this doesn’t happen the same way in every woman, and it’s not as predictable as people often say. Estrogen is part of the system that regulates stress, and shifting hormones can change how that system behaves.13
The hippocampus, the part of your brain that helps you form and retrieve memories, is very sensitive to cortisol. It’s packed with receptors that respond to stress hormones, so it’s one of the first places where changes in stress biology show up. In small, short bursts, cortisol can actually help. It sharpens focus and supports memory, like a bit of pressure that helps you perform. But when cortisol stays elevated for longer, the system gets uncalibrated. At that point, the brain begins to change in more structural ways. The connections between neurons become less complex (aka synaptic pruning), the creation of new neurons slows down, and the process that helps you lock in new information, what researchers call long-term potentiation, becomes less efficient. Over time, that shows up as very real memory issues, especially with recalling words, names, or recent conversations.
A helpful way to think about it is like a curve. Too little cortisol isn’t great, but too much for too long isn’t either. There’s a middle zone where the system works best, and outside of that, performance drops.
In human studies, this pattern holds up. Higher or chronically elevated cortisol levels are linked to worse memory and faster cognitive decline, and in conditions where cortisol is consistently high, like Cushing’s syndrome, broader cognitive problems are common. There’s also evidence that how sensitive your brain is to cortisol, even at a genetic level, can influence memory performance and even the structure of the hippocampus.3, 14
There are two kinds of stress your brain is dealing with. One is what you feel. The mental load, the sense of being overwhelmed, the pressure that’s always there in the background. The other is what your body is carrying quietly in the background, what researchers call allostatic load, which is the cumulative wear across systems like hormones, metabolism, inflammation, and the cardiovascular system.
What’s important is that both of these independently affect your brain. In long-term studies, people with higher perceived stress show worse cognitive performance over time, and the same is true for people with higher biological stress load. They run in parallel, not as one simple cause and effect.15
On the biological side, higher allostatic load is linked to changes in brain structure and performance, including memory, attention, and executive function. When the biological load combines with things like depression, the cognitive impact becomes more pronounced. This becomes especially relevant in perimenopause, because it’s a period where both types of stress tend to rise at the same time. Managing stress isn’t just about feeling better. It’s about protecting brain function.
Estrogen and progesterone do more than affect periods and hot flashes. They also help keep the brain’s immune system calmer and more controlled. One of the main players is the microglia, the brain’s built-in immune cells. When these cells get too activated, they release inflammatory signals like IL-1β, IL-6, and TNF-α, and those signals can interfere with how brain cells communicate, weaken the connections needed for learning and memory, and make thinking feel less sharp.
Estrogen helps put a brake on that process. It acts through several receptors in the brain and tends to push microglia toward a more protective, less inflammatory state. Progesterone and its metabolite allopregnanolone seem to help too, including protecting the blood-brain barrier, which is part of the brain’s defense system. So the overall idea is very plausible: when these hormones become less stable or start declining, the brain may lose some of that anti-inflammatory support, and that could make clear thinking harder. However, most of the strongest evidence for this pathway comes from animal studies and mechanistic models, not from direct human studies showing that perimenopausal hormone change leads step by step to everyday brain fog. So the biology of neuroinflamation makes sense, and many pieces of the pathway are well supported, but the full chain in humans has not been mapped cleanly yet.
Estrogen doesn’t just affect the brain directly. It also seems to shape the gut, and the gut can send signals back that influence mood, stress, sleep, and thinking. The microbiome talks to the brain through the immune system, hormones, metabolites, and even the vagus nerve, so when estrogen starts dropping, that whole conversation is affected.
Estrobolome is a group of gut bacteria involved in processing estrogen. Some of these bacteria help “unlock” estrogen in the gut so it can be reabsorbed and used again. If that system becomes less effective, which may happen after menopause or with gut dysbiosis, estrogen recycling can drop further. So it can become a loop: lower estrogen affects the gut, and changes in the gut may then make the estrogen picture worse.
Biologically, this makes sense, and it’s a compelling idea because estrogen is involved in so many brain functions, from neurotransmitters and mitochondria to blood flow and inflammation. But the honest answer is that the direct human proof is still limited. We have a strong mechanism, and we have enough pieces to take it seriously, but we do not yet have clean long-term studies in perimenopausal women showing that this gut-estrogen-brain pathway is a confirmed driver of cognitive symptoms.9
Menopause seems to affect the gut in ways that could matter for the brain. Studies suggest the gut microbiome becomes less diverse, and some of the bacteria that tend to drop are the ones that make short-chain fatty acids, or SCFAs. Those are small compounds that help keep the gut-brain system running smoothly. SCFAs help protect the blood-brain barrier, which is part of the brain’s security system, and they also help keep microglia, the brain’s immune cells, from becoming too reactive. When SCFA production drops, the brain may lose some of that protection and become more vulnerable to inflammation. There’s also a serotonin piece here. Most serotonin is made in the gut, and gut bacteria help regulate that process too, which means changes in the microbiome can potentially affect mood, stress signaling, and mental clarity.
So the overall chain makes sense: hormone changes can shift the gut, the gut may produce fewer protective compounds, and that can affect brain signaling. But we still do not have clean human proof showing this full step-by-step pathway causing cognitive symptoms in perimenopausal women.10,11
The six mechanisms above are at work in every perimenopausal woman. Four amplifying factors decide whether menopause brain fog stays manageable or starts costing you meetings.
Sleep disruption is one of the strongest amplifiers of menopause brain fog. Estrogen loss and poor sleep can both affect how your brain works. When sleep gets broken up, especially the deep slow-wave sleep your brain uses to encode and store memories, attention drops, reaction time slows, and memory works less efficiently the next day, even if you technically spent enough hours in bed. During that deep sleep, the hippocampus, your short-term memory center, transfers information to longer-term storage in the cortex, so when that stage is interrupted, the process could be incomplete.3
For many women, this is not an either-or problem. It’s not just hormones or just sleep. It’s both. Think of it like two separate hits to the same system: one changes how the brain functions during the day, and the other interrupts the nighttime work the brain needs to recover and lock in information. That’s why the effect can feel bigger than expected. Estrogen decline and sleep fragmentation can stack on top of each other, which helps explain why cognitive symptoms during this transition can feel so real and so persistent.16
Vasomotor symptoms with an important nuance. This is one of those findings that catches people off guard. The hot flashes you feel are not the ones most strongly linked to memory. It’s the ones your body is having at night, often without you even noticing.2
Women who have more of the nighttime hot flashes, measured using skin sensors, tend to perform worse on verbal memory tasks. But when you just ask women how many hot flashes they think they’re having, that link often disappears. The mechanism makes sense when you look at sleep. These nighttime flashes can briefly wake the brain, even if you don’t fully remember it. That’s the stage your brain uses to consolidate memories, especially verbal ones. At the same time, these events can trigger small stress responses, including cortisol spikes, right when cortisol is supposed to be low.
So you end up with repeated interruptions during the exact window when your brain is trying to store information. Think of it like trying to save a document while someone keeps unplugging your computer for a few seconds at a time. You might not notice every interruption, but the final file isn’t as complete. That’s why objective nighttime hot flashes seem to track memory changes better. They’re capturing the physiological disruption, not just what you remember experiencing.
Anxiety and depression can intensify menopause brain fog. SWAN study showed that women in perimenopause show measurable changes in cognitive function, things like slower processing speed and slightly reduced learning compared to their own earlier baseline. Depression and anxiety each add their own layer to what’s happening in the brain during this transition. Depressive symptoms are consistently linked to more memory complaints and weaker working memory, especially when it comes to holding and encoding new information. They also tend to slow processing speed, which can make the underlying perimenopause-related changes feel more noticeable. Part of this comes down to brain chemistry. Depression affects systems like serotonin and dopamine, which are involved in focus and motivation, and it also interacts with sleep and stress pathways that the brain relies on for clear thinking.
Anxiety shows up a little differently. It’s quite common in perimenopause and can affect how efficiently you learn and recall information, especially verbal and episodic memory. Mechanistically, anxiety keeps the brain in a more alert, threat-focused state, pulling resources away from memory and concentration. Over time, especially if stress is ongoing, that constant “on edge” signal can make cognitive symptoms feel more persistent. These are not the root cause of the transition, but they do layer on top of it and can make the experience feel heavier and more unpredictable.17
High cognitive load can make menopause brain fog significantly more noticeable. There’s another layer to brain fog that has nothing to do with hormones directly, and that’s the overall load you’re carrying in your life. Things like irritability, low mood, feeling stretched too thin, financial pressure, or not feeling valued at work don’t just sit in the background. They raise your perceived stress, and that alone is strongly linked to problems with memory and concentration in midlife women. When your system feels constantly under pressure, attention becomes less stable and everything starts to feel mentally heavier. Research estimates around 60% of perimenopausal women report cognitive changes that directly affect work performance, with 47% reporting brain fog has affected a critical work decision in the past year.3
Part of this is how the brain prioritizes resources. Under stress, it shifts toward managing what feels urgent or threatening and pulls energy away from things like memory and focus. Add fatigue, poor sleep, or feeling generally unwell, and that effect compounds. So even if the hormonal transition is setting the baseline, this psychosocial load can turn something subtle into something much more noticeable. Brain fog in this stage is not just hormonal. It’s hormonal plus load. The biology sets the stage, and the life context can either amplify it or soften it.
Brain fog tends to be at its worst during perimenopause and the early postmenopause phase, which is the period when hormones are the most unstable. That’s when women show the biggest dips in verbal memory, processing speed, and attention, and it’s also when subjective complaints, that “something feels off” feeling, are most common. As things settle into a more stable low-hormone state later on, cognitive performance often improves again toward earlier levels. In large longitudinal studies like SWAN, women tend to show a dip in things like verbal memory and processing speed during perimenopause, and then those functions improve again in early postmenopause, often returning close to where they were before.3
What matters more than your exact age is where you are in the transition. Two women can both be 48, but if one is still hormonally stable and the other is deep in perimenopause, their brain function can feel very different. During this transition, the brain shows changes in energy use and connectivity, especially in memory-related and frontal regions, and those changes track with hormone fluctuations and cognitive performance.
What brain imaging shows is a bit more reassuring than most of us would expect but also more nuanced. During the transition, the brain does go through measurable changes. Gray matter volume in areas important for memory and thinking can decrease, and the brain’s energy use becomes less efficient. That’s the phase where things feel the most unstable, because the system is actively adjusting. But after menopause, there are signs of partial recovery. Some of that gray matter loss reverses in key regions, and brain networks look more organized again. This recovery is even linked to better cognitive performance and improved energy production in brain cells, which suggests the brain is adapting, not just declining. At the same time, it doesn’t go fully back to the exact premenopausal state. Brain metabolism often remains somewhat altered, meaning the system is more stable, but not identical to before. You can think of it like a system that has reconfigured itself. It finds a new steady state, but it’s not the original one.4
So the overall pattern is this: the transition is the most dynamic and challenging phase, followed by a period of stabilization with some recovery. For many women, menopause brain fog improves in postmenopause. But how complete that recovery is depends on the individual, and for some women, underlying vulnerabilities like metabolic or cardiovascular health can still shape longer-term brain risk.
The good news is, it’s a window of vulnerability when you can intervene!
No single intervention can address all six mechanisms. Managing menopause brain fog requires a layered approach. The layers do not carry equal evidence strength, which matters for prioritizing.
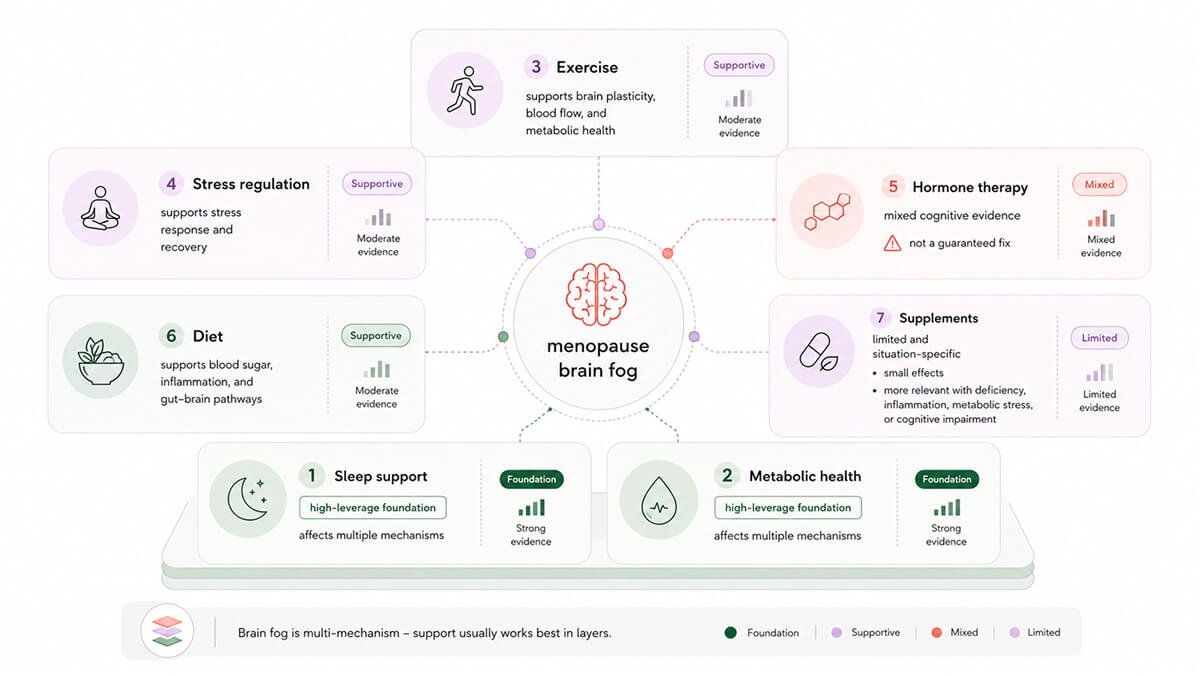
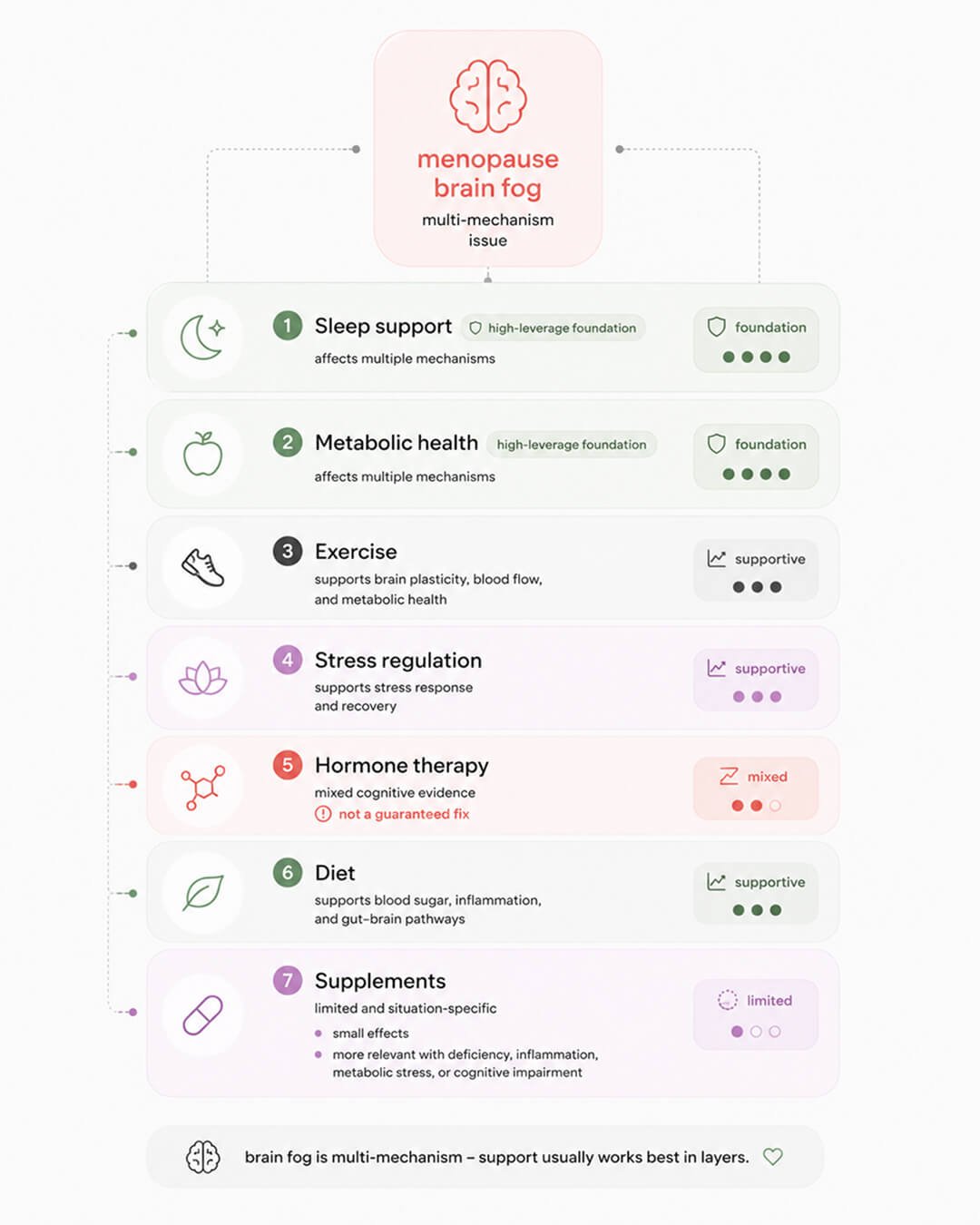
Hormonal therapy has mixed effects on menopause brain fog. When it comes to hormone replacement therapy (HRT) and cognition, the honest answer is: it’s not a magic fix. Overall, human studies show mostly neutral to small cognitive effects. Standard menopausal hormone therapy does not reliably make women think sharper across the board, but it also does not seem broadly harmful when started around the menopause transition.6
Exercise can ease menopause brain fog, but not every type has the same evidence behind it. Progressive resistance training looks promising for cognition, though most of the research is in older adults, not perimenopausal or postmenopausal women specifically.
The studies we do have show that lifting 2 to 3 times a week for a few months can improve processing speed, focus, and executive function (the thinking you use to plan, switch tasks, and hold several projects in your head at once). Gains appear larger when strength work is paired with aerobic exercise, whether that’s walking, intervals, or anything that keeps you moving.18
Mechanistically, this makes sense. Resistance training doesn’t just build muscle. It also sends signals to the brain through neurotrophic factors, myokines, blood flow, and nervous system activation. BDNF gets a lot of attention because it helps support neuroplasticity, which is the brain’s ability to adapt, strengthen connections, and learn. You can think of exercise as making the brain more ready to change.
Interestingly, if you add cognitive challenge at the same time, you may be able to direct that plasticity more specifically. In other words, exercise may open the window, and the mental challenge may tell the brain where to build. But when it comes to perimenopause specifically, the evidence is still thin. We do have studies showing resistance training is safe and effective for strength in midlife women, but the dedicated trials looking at cognition in perimenopausal women are still largely missing.
Diet’s influence on menopause brain fog is harder to pin down than the exercise evidence. The two dietary patterns with the strongest cognitive data are Mediterranean and MIND (a Mediterranean-DASH hybrid built specifically for brain health), but again, most of the research is in older adults, not perimenopausal women.
The observational data for MIND is striking. In Morris et al.’s landmark 2015 cohort, the gap between the highest and lowest MIND adherers was equivalent to 7.5 years of cognitive aging.23
The randomized trials tell a messier story. A small 3-month MIND trial in 40 overweight women improved verbal learning and recognition memory, though it showed no effect on executive function.21 The larger 2023 MIND trial with 604 participants over three years found no significant difference between MIND and a control diet. Both groups improved modestly, likely because both included mild calorie restriction and weight loss.22
The Mediterranean diet has stronger trial backing. In long-term studies like PREDIMED, a Mediterranean pattern with extra-virgin olive oil improved global and frontal cognition and reduced the risk of mild cognitive impairment over about 4 to 6 years.
Mechanistically, both diets help stabilize blood sugar, which the brain depends on. They reduce inflammation and oxidative stress through foods like olive oil, berries, nuts, and fish. And they support the gut microbiome through fiber, which may influence brain signaling and inflammation as well as we have already discussed. They are not a guaranteed protection, and they work best as part of a broader picture rather than as a single intervention.
Supplements and menopause brain fog. So far, the best direct data for using 1.5 g/day creatine hydrochloride for brain fog comes from one randomized clinical trial (RCT) in perimenopausal and postmenopausal women. In that study, creatine hydrochloride for 8 weeks led to faster reaction time and increased frontal brain creatine by roughly 16% vs. placebo. There’s also a smaller study combining creatine with strength training that showed improvements in strength and sleep, but it didn’t show clear cognitive gains on formal testing.19
Mechanistically, the story is quite clean. Creatine becomes phosphocreatine in the brain, which acts like a rapid energy buffer. When your neurons need ATP quickly, for focus, working memory, processing speed, that system helps keep things running smoothly. This seems especially relevant in states where brain energy is under pressure, like aging, sleep disruption, or hormonal transition.
There are other supplements that show very modest cognitive benefit and they work best in specific situations rather than helping with brain fog.20
Polyphenols like curcumin, cocoa flavanols, green tea, and berry compounds have been shown to slightly improve memory, attention, and mood in older adults with mild memory concerns. The mechanism is fairly straightforward. They reduce inflammation, improve blood flow to the brain, and support cellular resilience.
Vitamins and omega-3s show a similar pattern. B vitamins like folate, B6, and B12, along with vitamin D, can improve cognition, but mainly when there is a deficiency or elevated homocysteine. Omega-3s can modestly support memory and attention, but large trials in generally healthy adults are mixed.
Multi-ingredient formulas tend to show the largest effects, especially in people with mild cognitive impairment or early Alzheimer’s. These combinations often include B vitamins, omega-3s, antioxidants, and sometimes phospholipids. Part of their effect seems to come from lowering inflammation, for example reducing markers like CRP. But it’s hard to isolate what is doing what, and these are typically studied in populations already showing decline.
Then there’s the gut angle. Certain probiotic strains, like Bifidobacterium breve A1 or Lactobacillus plantarum C29, have been shown to improve cognitive scores, attention, and even mood in older adults with mild impairment. These effects seem to run through gut-brain signaling and factors like BDNF.
These supplements can somewhat help, but mostly in people who have an underlying condition, inflammation, deficiency, metabolic stress, or early cognitive impairment. The effects are usually small, and they don’t translate cleanly into “this will fix brain fog” for a woman in perimenopause or postmenopause.
If you’re not sure where to start on improving menopause brain fog, focus on sleep and metabolic health. Between them, they touch more of the six mechanisms than any other intervention, and neither requires a prescription or a specialist referral. You can start tonight.
Menopause brain fog is not you losing your edge. It is your brain running a different operating system without a manual.
What causes menopause brain fog is not one thing; it is six overlapping mechanisms, and the estrogen brain fog story is only the beginning. Perimenopause concentration problems, menopause memory problems, the word that disappears mid-sentence – these are not personality failures or signs of early decline. They are predictable biological consequences of a hormonal transition that science has under-researched for decades.
The good news is that menopause brain fog relief is not a mystery. The research on brain fog menopause treatment is newer than it should be, but it is moving fast. Some of the studies cited here are less than twelve months old. We are not at the end of what science will tell us about perimenopause brain fog. We are somewhere in the middle. And the middle is a much better place to be than where we were ten years ago.
I know the feeling well, I’m in perimenopause myself. I have changed how I structure my weeks, how I protect my effective hours, and how much I expect from myself on the days that feel heavier.
Dr. Jura Lasas
1.
Bangle, A. et al. Cognitive Functioning in Perimenopause: An Updated Systematic Review and Meta-Analysis (2026) https://doi.org/10.1037/pag0000946
2.
Weber, M. T. et al. Cognitive profiles in perimenopause: hormonal and menopausal symptom correlates (2021) https://doi.org/10.1080/13697137.2021.1892626
3.
Metcalf, C. A. et al. Cognitive Problems in Perimenopause: A Review of Recent Evidence (2023) https://doi.org/10.1007/s11920-023-01447-3
4.
Mosconi, L. et al. Menopause impacts human brain structure, connectivity, energy metabolism, and amyloid-beta deposition (2021) https://doi.org/10.1038/s41598-021-90084-y
5.
Jett, S. et al. Sex and menopause impact 31P-Magnetic Resonance Spectroscopy brain mitochondrial function in association with amyloid-beta load (2022) https://doi.org/10.1038/s41598-022-26573-5
6.
Puri, T. A. et al. Association Between Menopause Age and Estradiol-Based Hormone Therapy With Cognitive Performance in Cognitively Normal Women in the CLSA (2025) https://doi.org/10.1212/WNL.0000000000213995
7.
Luo, C. et al. Sex-specific associations between estimated glucose disposal rate and cognitive decline in middle-aged and older adults in China: a longitudinal cohort study (2025) https://doi.org/10.3389/fnagi.2025.1544352
8.
Mruczyk, K. et al. The Role of Inflammatory Markers in Linking Metabolic Syndrome to Cognitive Decline in Middle-Aged Women: A Focus on TNF-α and IL-6 (2025) https://doi.org/10.3390/metabo15030186
9.
Cuozzo, M. et al. Gut-brain communication in menopause: insights into neuroendocrine and microbiome interactions (2026) https://doi.org/10.1017/s0029665126102201
10.
Peters, B. A. et al. Spotlight on the Gut Microbiome in Menopause: Current Insights (2022) https://doi.org/10.2147/ijwh.s340491
11.
Guo, C. et al. Effects of a healthy diet based on seed-rich vegetables on the gut microbiota and intrinsic brain activity in perimenopausal women: A pilot study on cognitive improvement (2025) https://doi.org/10.1038/s41598-025-99406-w
12.
Coelho-Júnior, H. J. et al. Effects of Combined Resistance and Power Training on Cognitive Function in Older Women: A Randomized Controlled Trial (2020) https://doi.org/10.3390/ijerph17103435
13.
James, K. A. et al. Understanding the relationships between physiological and psychosocial stress, cortisol and cognition (2023) https://doi.org/10.3389/fendo.2023.1085950
14.
Kim, E. J. et al. Neurocognitive effects of stress: a metaparadigm perspective (2023) https://doi.org/10.1038/s41380-023-01986-4
15.
De Looze, C. et al. Mind versus body: Perceived stress and biological stress are independently related to cognitive decline (2023) https://doi.org/10.1016/j.bbi.2023.10.017
16.
Grant, L. K. et al. The effect of experimentally induced sleep fragmentation and estradiol suppression on neurobehavioral performance and subjective sleepiness in premenopausal women (2024) https://doi.org/10.1093/sleep/zsae130
17.
Greendale, G. A. et al. Menopause-associated Symptoms and Cognitive Performance: Results From the Study of Women’s Health Across the Nation (2010) https://doi.org/10.1093/aje/kwq067
18.
Macaulay, T. R. et al. 12 weeks of strength training improves fluid cognition in older adults: A nonrandomized pilot trial (2021) https://doi.org/10.1371/journal.pone.0255018
19.
Korovljev, D. et al. The Effects of 8-Week Creatine Hydrochloride and Creatine Ethyl Ester Supplementation on Cognition, Clinical Outcomes, and Brain Creatine Levels in Perimenopausal and Menopausal Women (CONCRET-MENOPA): A Randomized Controlled Trial (2025) https://doi.org/10.1080/27697061.2025.2551184
20.
Fekete, M. et al. Improving Cognitive Function with Nutritional Supplements in Aging: A Comprehensive Narrative Review of Clinical Studies Investigating the Effects of Vitamins, Minerals, Antioxidants, and Other Dietary Supplements (2023) https://doi.org/10.3390/nu15245116
21.
Charbit, J. et al. Effects of Dietary Interventions on Cognitive Outcomes (2025) https://doi.org/10.3390/nu17121964
22.
Barnes, L. L. et al. Trial of the MIND Diet for Prevention of Cognitive Decline in Older Persons (2023) https://doi.org/10.1056/NEJMoa2302368
23.
Morris, M. C. et al. MIND diet slows cognitive decline with aging (2015) https://doi.org/10.1016/j.jalz.2015.04.011

Mood & Energy Solutions

Fatigue Causes & Types
Fatigue Causes & Types

Workplace Strategies

Menopause at Work

Brain Fog at Work

Brain Fog at Work

Is This Perimenopause?

Is This Perimenopause?

Nutrition & Supplements

Workplace Strategies

Menopause Science

Menopause Science

Brain Fog Solutions
We use cookies and similar technologies to ensure the proper functioning of our website, personalize content, provide social media features, and analyze traffic. By clicking “I Agree”, you consent to the use of these technologies.
No results




