22 June 2026
What Does Menopause Brain Fog Symptoms Feel Like at Work?

Reading time 13 min.

Reading time 13 min.
You have twenty-five years of expertise in your field. You have sat in rooms where you were the smartest person there. And this morning you could not remember the word for the thing you have spent those twenty-five years working on. It came back four hours later, in the car: “database.” Menopause brain fog symptoms are narrow, specific, almost absurd. The general sense is “I’m off, my thinking is not the same.” Brain fog does not touch what you know. Menopause brain fog symptoms touch only your ability to get to that knowledge.
Menopause brain fog symptoms arrive as patterns, not as a single problem. “Brain fog” is not a medical diagnosis. The phrase is shorthand for a specific set of cognitive experiences. When researchers break the label apart, two patterns emerge:
A tool called the Everyday Memory Questionnaire separates retrieval from attention. When researchers used the questionnaire in more than 400 women going through menopause, retrieval problems were highest in perimenopause. Attention scores barely shifted across menopause stages. The finding is specific: brain fog is not a general decline in your thinking. Brain fog is a problem of access to information you already know. Your brain still has the file, but the search function is slower or less precise.1 Menopause brain fog symptoms affect access, not intelligence.
What women describe as “brain fog” during perimenopause often comes down to one specific problem: verbal memory retrieval. The information is there, but access becomes unreliable. A 2017 study tested adults aged 45 to 55 and found women still outperformed men across memory tasks, but that advantage narrowed after menopause.3 When the researchers broke memory into components, the pattern became clear. Initial learning and pulling information on demand weaken first. Storage and consolidation remain intact. It helps to think of it as a filing system that still stores everything correctly, but the indexing becomes inconsistent, especially when you are under time pressure or cognitive load.
Word-finding failure tends to surface most clearly in professional settings, especially in moments where you are expected to respond quickly and precisely. In neuroscience, this is described as a tip-of-the-tongue state. The issue is not that the word or concept is gone. The meaning is fully accessible. What fails is the retrieval of the sound pattern of the word, a phonological access problem rather than a loss of knowledge.4
Research shows that being observed and evaluated increases tip-of-the-tongue rates significantly across adults of all ages. Under scrutiny, the brain becomes less efficient at converting meaning into spoken language. In a meeting, where attention is divided and stakes are visible, this shift becomes noticeable. In perimenopause, retrieval is already less stable due to hormonal effects on brain signaling and network efficiency. When a high-visibility situation adds pressure, the system is asked to perform under two constraints at once.
Sustained attention is where the second problematic pattern shows up. You stay in the meeting, but it’s difficult to follow. Multiple voices become harder to track. You read the same paragraph again because it did not fully register the first time. The issue is not effort. It is the brain’s ability to hold and process incoming information in real time.
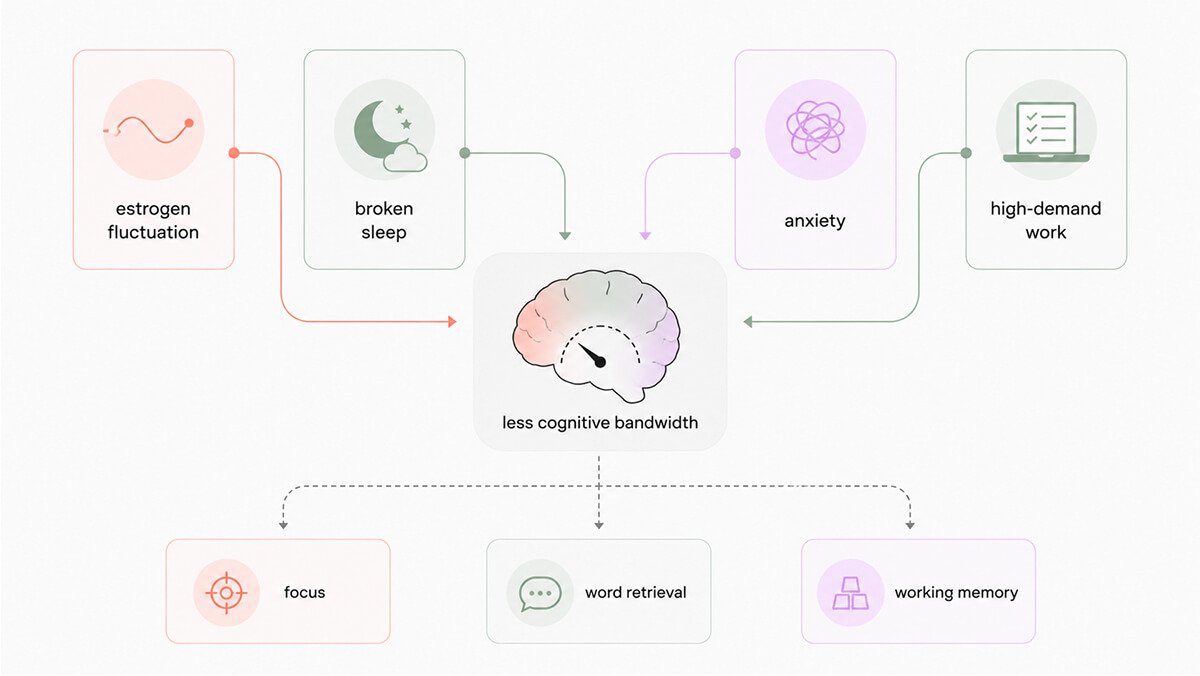
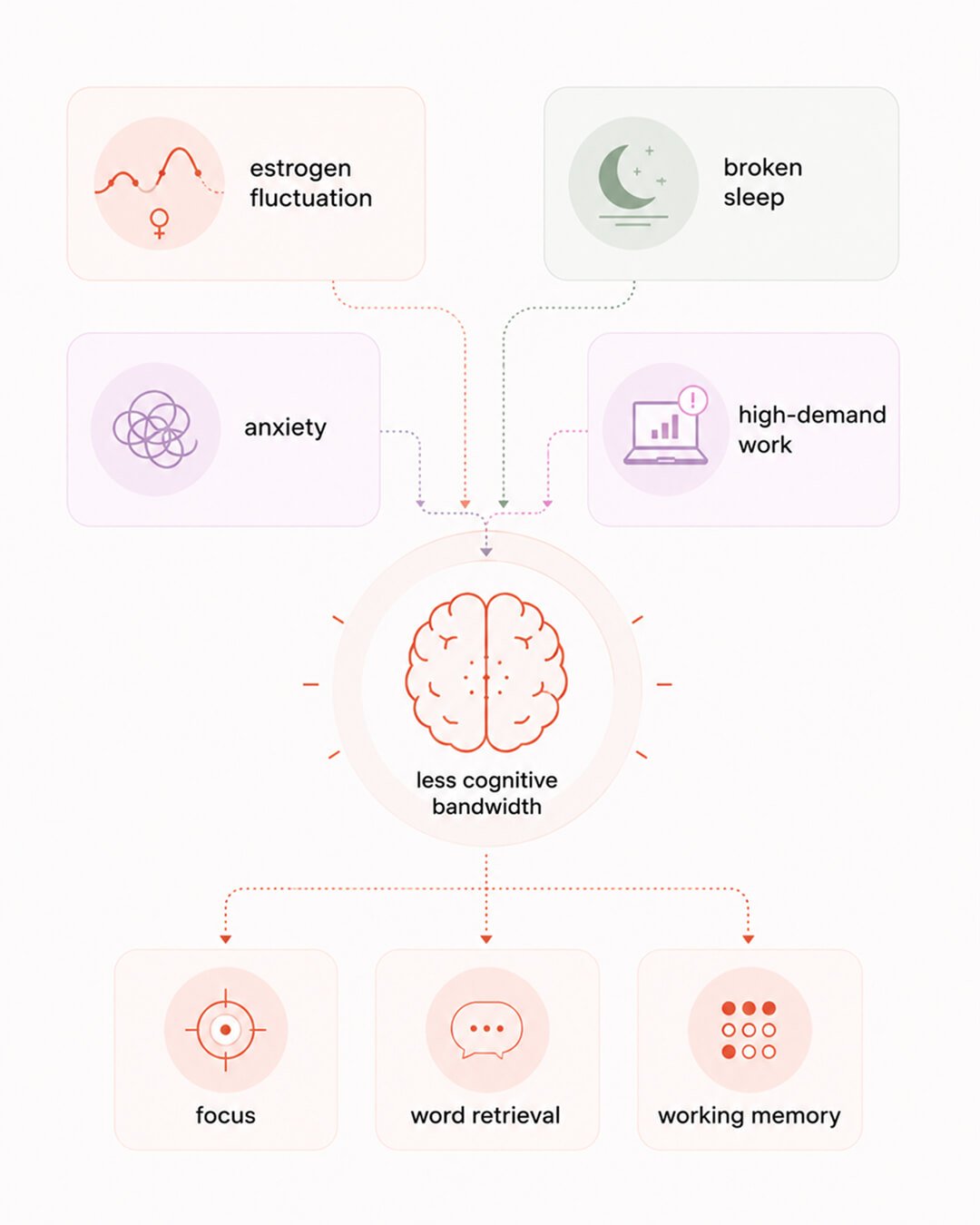
A 2023 study followed 43 women over 12 weeks, measuring estrogen metabolites weekly alongside cognitive testing. Within the same woman, higher-estrogen days aligned with better attentional performance and fewer memory complaints. On lower-estrogen days, auditory information was less likely to register on the first pass. Your ability to pay attention shifts day to day because estrogen levels are shifting day to day. Perimenopause is defined by irregular estrogen fluctuation, not a steady decline. Attention shifts with hormone changes, so the same task can feel clear one day and effortful the next, without anything around you changing.5
Cognitive fatigue follows a predictable pattern across the workday. Interviews with women show mental effort is already elevated in the morning and builds with each cognitively demanding task, especially after multitasking, context switching, or fragmented sleep. The change during perimenopause is in cognitive bandwidth under load, not in how capable you are. Prefrontal brain networks that manage attention and task coordination require more energy to maintain the same level of performance. Tasks that once ran automatically, such as leading a meeting, reading email, tracking multiple action items, now require deliberate attention at each step. Performance stays intact, but it requires more effort to maintain.6
Symptoms that come and go create a different problem than the symptoms themselves. Some hours feel sharp. Other hours require more effort for the same task. Estrogen levels during perimenopause fluctuate rather than decline steadily. Within the same woman, higher estrogen levels align with stronger attention and memory, while lower levels make information harder to register and hold. Performance becomes difficult to predict because cognitive function follows those shifts rather than staying stable across the day.
Sleep is the clearest amplifier of perimenopause brain fog. A 2024 experimental study in Sleep tested two conditions in premenopausal women: broken sleep that mimics menopause patterns without reducing total sleep time and lowered estrogen levels using medication. Broken sleep increased attentional lapses by 0.6 events and slowed reaction time by 9.4 milliseconds, while lowered estrogen increased lapses by 0.8 and slowed reaction time by 12.3 milliseconds. The effects add together.7
Broken sleep reduces the brain’s overnight recovery of attention. Lower estrogen changes signaling in brain regions that support focus and working memory. When both occur in the same night, the brain starts the next day with less restored capacity and less efficient processing. You notice attention slipping faster and responses taking longer, especially under pressure.
Perimenopause disrupts sleep mainly by breaking it apart, not by shortening it. Night sweats and brief awakenings interrupt the sequence of deep and REM sleep that rebuilds memory and attention. The brain misses the stages that stabilize information and reset focus for the next day.
Anxiety and low mood often show up alongside brain fog during perimenopause, but they are not the sole cause of cognitive problems. Hormonal changes affect both emotional regulation and the brain regions responsible for attention, working memory, and mental flexibility. The same biological shift can make you feel more anxious and less mentally sharp at the same time. Cognitive symptoms can appear even when mood feels stable.
Anxiety adds a second layer. Attention turns inward toward worry and monitoring, leaving less capacity for the task in front of you. Information does not register as cleanly and is harder to hold and retrieve. Low mood works differently. Processing slows, mental energy drops, and effort increases for the same output. You notice this as difficulty organizing thoughts, losing track of steps, or struggling to stay engaged.
The anxiety component can be reduced even while the hormonal transition continues. Psychological approaches such as cognitive behavioral therapy and mindfulness reduce anxiety and low mood and are linked to fewer memory and attention complaints. The hormonal driver may still be present, but lowering anxiety frees up mental capacity. The work feels more manageable, even when the biology has not fully settled.8
High-demand work situations expose even small changes in cognitive efficiency. The functions under the most pressure during perimenopause are rapid word retrieval, sustained attention, verbal fluency under observation, and tracking multiple threads at once. These are the same functions senior roles rely on every day. A small drop in speed or stability becomes visible because the margin for error is low. You feel this as needing more effort to keep up in meetings, losing a word at the wrong moment, or struggling to hold several inputs in mind while responding.
Workplace data reflect this pattern. Poor concentration and memory are the cognitive symptoms most often reported as affecting performance more than half of the time, and these cognitive and psychological symptoms are reported more often than hot flashes in work settings. Hot flashes are easier to see and easier to discuss. Concentration and memory are less visible, but they carry the greater cost because they are at the center of how work gets done.9
A 2025 meta-analysis looked across more than 5,000 women and compared subjective complaints with objective cognitive tests. The link between the two was surprisingly weak. Across memory, attention, and executive function, standard tests often didn’t pick up what women were clearly experiencing. It doesn’t mean the symptoms aren’t real. It means the tools we use to measure cognition were not designed to capture this kind of change. So you end up in a situation where you feel a very real shift in how your brain is working, especially in high-demand, real-world situations, and the formal testing environment doesn’t fully reflect it. It explains why so many women say, “Something is off,” while being told everything looks normal.2
Cognitive changes during perimenopause do not follow a single pattern. Data collected from the same women over time show several distinct profiles: most women remain cognitively stable, some show specific weaknesses in verbal learning and memory, and others show strengths in attention or executive function. The group that showed cognitive weaknesses was not older and did not start with lower ability. The difference came down to that they were sleeping worse and their estrogen levels were flatter and lower. Brain fog does not follow a single pattern. The group showing specific cognitive changes was tied to sleep and hormone patterns, not just where they are in menopause transition.
A 2015 randomized clinical trial tested lisdexamfetamine, a stimulant medication used in ADHD, in 32 healthy women in late perimenopause or early menopause who reported new problems with focus and mental control but had never had ADHD. The medication improved how women experienced their thinking subjectively. Scores for organization, sustained attention, mental effort, processing speed, and working memory all improved compared to placebo. On objective testing, only one measure improved, delayed recall of a short story, while other cognitive tests stayed the same. What women feel is not a loss of ability but a loss of consistency in accessing that ability. The medication appears to reduce that internal effort and make performance feel more steady again. How? Estrogen helps keep dopamine signaling stable in the prefrontal cortex, which supports focus, planning, and working memory. When estrogen becomes unstable, dopamine signaling also becomes less consistent, and lisdexamfetamine raises dopamine levels to help restore more reliable executive function.10
Perimenopause brain fog symptoms do not just affect getting work done. It changes how you see yourself at work. Studies and interviews show a clear split between what women know they can do and how capable they feel in high-visibility moments. More than half of working women in menopause worry others will see them as less competent because of these symptoms.11
Performance data does not show a matching drop. Most women stay within normal range, but internal feedback becomes negative in moments when judgment matters. The brain signals “something is off” even when output holds steady. That mismatch makes women hesitate to step into visible roles, not because ability changed, but because confidence drops exactly when it is needed.
The pattern tracks with cognitive and psychological symptoms, not physical ones. Hot flashes and joint pain do not drive this shift. Changes in attention, mental effort, and self-perception do. One study described women engaging in “contradictory behaviors at work.” They stay outwardly sharp and dependable while privately questioning their own competence. This reflects a brain that is maintaining performance under higher internal strain.12
Workplace policies tend to focus on visible physical symptoms. The real career impact is in hidden cognitive changes that shape how a woman evaluates her own performance.
The research on perimenopause brain fog keeps returning to the same finding: retrieval is the problem, not storage. What you know is intact. Getting to it under pressure, on demand, in the middle of a meeting where everyone is waiting, that’s where the friction is. The filing system still works. The indexing got messed up. The expertise you’ve spent decades building isn’t going anywhere. The access to it has become less automatic and we can work with that change.
What I find harder to shake is the split between how women are performing and how they feel they’re performing. The research shows most women stay within the normal range. But the internal dialogue tells them something different in the moments when confidence matters most. That gap has real career consequences, not because ability changed but because the inner critic got louder. Your brain is navigating a major reorganization; be gentle with yourself. Science is on your side, you aren’t losing your abilities.
Dr. Jura Lasas
1.
Zhu, C. et al. Evaluation of the Everyday Memory Questionnaire-Revised in a menopausal population: understanding the brain fog during menopause (2023) https://doi.org/10.1097/GME.0000000000002256
2.
Furey, R. T. et al. Subjective versus objective cognition during menopause: A systematic review and meta-analysis (2025) https://doi.org/10.1017/s1355617725101306
3.
Rentz, D. M. et al. Sex differences in episodic memory in early midlife: impact of reproductive aging (2017) https://doi.org/10.1097/GME.0000000000000771
4.
Burke, D. M. et al. On the tip of the tongue: What causes word finding failures in young and older adults? (1991) https://doi.org/10.1016/0749-596X(91)90026-G
5.
Grummisch, J. A. et al. Within-person changes in reproductive hormones and cognition in the menopause transition (2003) https://doi.org/10.1016/j.maturitas.2023.107804
6.
Kunasegaran, K. et al. Understanding mental fatigue and its detection: a comparative analysis of assessments and tools (2023) https://doi.org/10.7717/peerj.15744
7.
Grant, L. K. et al. The effect of experimentally induced sleep fragmentation and estradiol suppression on neurobehavioral performance and subjective sleepiness in premenopausal women (2024) https://doi.org/10.1093/sleep/zsae130
8.
Coslov, N. et al. “Not feeling like myself” in perimenopause — what does it mean? Observations from the Women Living Better survey (2024) https://doi.org/10.1097/GME.0000000000002339
9.
O’Neill, M. T. et al. Impact of menopausal symptoms on work and careers: a cross-sectional study (2023) https://doi.org/10.1093/occmed/kqad078
10.
Epperson, C. N. et al. New onset executive function difficulties at menopause: a possible role for lisdexamfetamine (2015) https://doi.org/10.1007/s00213-015-3953-7
11.
Smith, W. et al. The influence of menopause symptoms on workplace mental health among Irish women: A preliminary study (2025) https://doi.org/10.1016/j.cpnec.2025.100324
12.
Steffan, B. Managing menopause at work: The contradictory nature of identity talk (2020) https://doi.org/10.1111/gwao.12539

Mood & Energy Solutions

Fatigue Causes & Types
Fatigue Causes & Types

Workplace Strategies

Menopause at Work
Brain Fog at Work

Brain Fog at Work

Is This Perimenopause?

Is This Perimenopause?

Nutrition & Supplements

Workplace Strategies

Menopause Science

Menopause Science

Brain Fog Solutions
We use cookies and similar technologies to ensure the proper functioning of our website, personalize content, provide social media features, and analyze traffic. By clicking “I Agree”, you consent to the use of these technologies.
No results





