22 June 2026
Perimenopause at Work: How Hormonal Changes Affect Executive Performance

Reading time 16 min.

Reading time 16 min.
You feel it before you can name it. A word slips mid-sentence in a meeting where you have made the same kind of argument a hundred times. A colleague references something you said last week, and you cannot quite place it. You start doubting yourself. The data on perimenopause at work is now clear: the cognitive complaints during this transition are real, biologically grounded, and especially noticeable in executive roles where working memory and verbal fluency are essential.1,2 However, most of these changes are temporary.3 A growing body of evidence-based interventions can protect your cognitive performance through this phase.4 While menopause at work doesn’t have to mean a career plateau, it does require understanding what is happening in your brain and acting on the evidence.
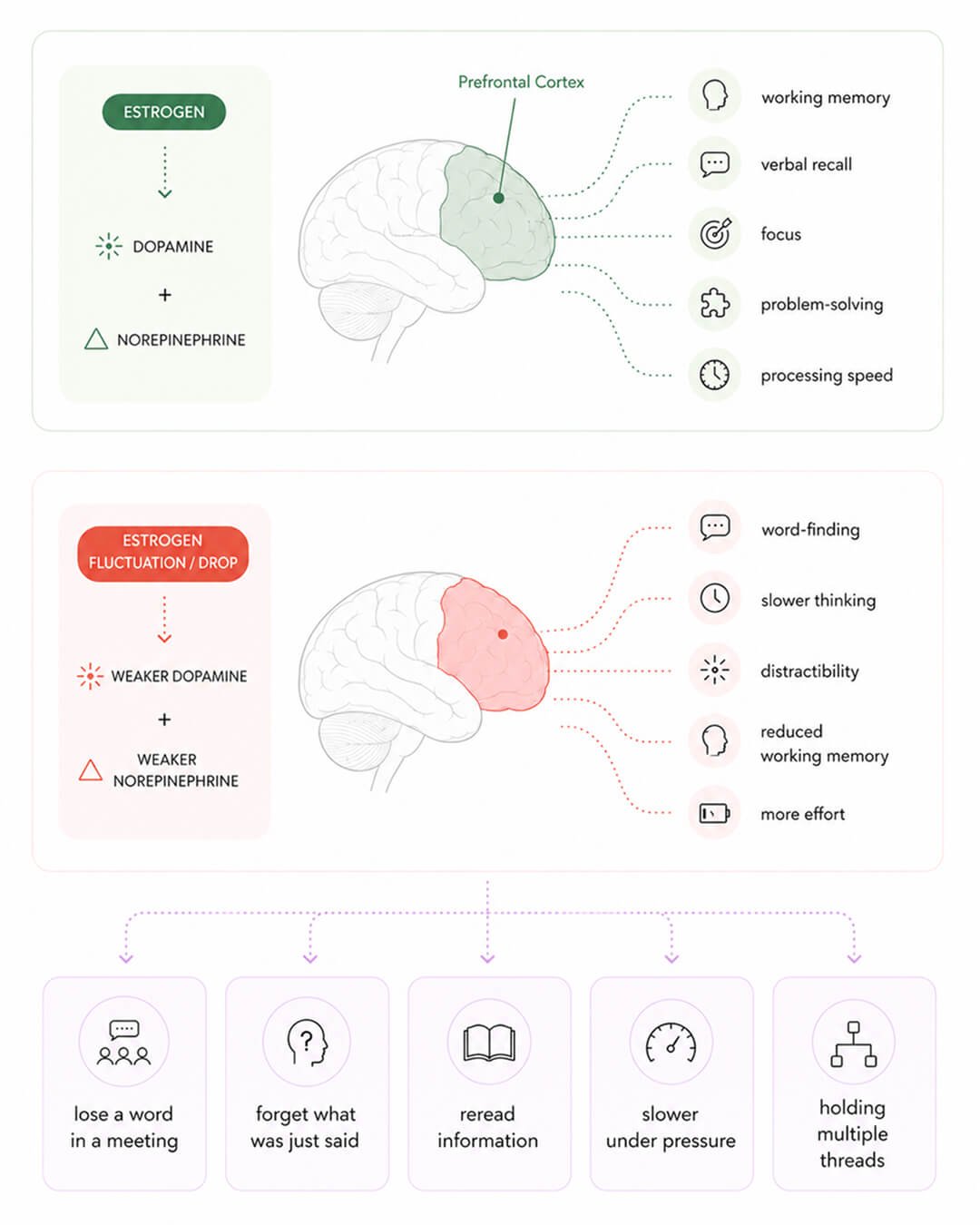
Estrogen is not only a reproductive hormone. In your brain, it acts as a vital signaling molecule. The prefrontal cortex, the region located behind your forehead that manages complex judgment, problem-solving, and verbal recall, is densely packed with estrogen receptors.5,6
Estrogen works in tandem with two essential brain chemicals in your prefrontal cortex: dopamine and norepinephrine. Dopamine regulates your level of focus, motivation, and sustained working memory, while norepinephrine sharpens your attention and helps you maintain your train of thought despite interruptions. Estrogen amplifies both of these signals. Consequently, when estrogen levels drop, both dopamine and norepinephrine signals weaken, leaving your prefrontal cortex with fewer resources to function effectively.6,7,8
Your brain does not take this decline passively. As estrogen levels fall, your brain actually compensates by increasing the density of estrogen receptors in regions tied to memory and complex thinking. When this compensation is successful, your cognitive performance remains steady. However, when it falls short, the gap manifests as the symptoms you may have started to notice.9
Long-term studies, including the Study of Women’s Health Across the Nation (SWAN), have mapped which cognitive areas are most affected during perimenopause.3,10 The most consistent changes are in verbal memory (remembering specific events and words), working memory (holding and using information in real time), and processing speed (how fast you process information).12 The drops are small to moderate, but in a meeting where seconds count, even small drops seem noticeable.

The Mayo Clinic conducted the largest survey yet on menopause in the workplace, finding that women with the most severe symptoms were over 15 times more likely to experience negative career impacts. Nationally, this results in an estimated $1.8 billion in annual losses in the U.S. alone.11 Similarly, an Irish study revealed that 65% of women felt their job performance suffered, citing poor concentration and memory as their primary challenges.12 Furthermore, a 2025 study of 3,500 Latin American women confirmed that severe symptoms are a direct predictor of job loss, early retirement, and decreased productivity.13
The data across these studies points to a clear trend: it isn’t just “being in menopause” that affects your career, but rather how severe your symptoms are.13,14 The specific issues that interfere most with work are cognitive and psychological, such as struggling to find the right words, memory lapses, slower thinking, and the anxiety that arises when these moments happen during high-pressure tasks.15,16,17
There is often a disconnect between how you feel and what cognitive tests actually show. While brain fog in perimenopause is common, your subjective experience is often more severe than what formal testing picks up.2 The reason for this gap is important: issues like disrupted sleep, the high cortisol levels caused by stress, and symptoms of depression all make brain fog feel much worse than estrogen loss would on its own.18,19 In many cases, once you address sleep and mood, the “foggy” feeling begins to lift even before you target the brain directly.
The overlap between perimenopause and ADHD is significant and worth understanding. Estrogen helps regulate dopamine and norepinephrine in your prefrontal cortex – the same brain chemicals targeted by ADHD medications. When estrogen levels drop sharply, these chemical signals weaken, leading to symptoms that look exactly like ADHD: distractibility, trouble starting tasks, memory lapses, and difficulty managing emotions.7,8
The distinction between the two depends largely on your history:
Understanding this difference is crucial because the treatment approaches for hormonal changes versus neurodevelopmental ADHD are different.
The most important point often gets overlooked: the cognitive changes you experience during perimenopause are not the beginning of a long-term decline. Long-term studies show that the most challenging phase is perimenopause itself, rather than the years that follow. In fact, once you reach postmenopause, your processing speed, working memory, and visual memory typically improve compared to where they were in premenopause.3,10 Your brain is not failing; it is reorganizing.
You also carry a second protective factor that you may not realize. Cognitive reserve is your brain’s ability to maintain performance despite biological changes, and it is built by years of demanding intellectual work. A large UK Biobank study found that higher cognitive reserve predicted slower cognitive decline in midlife and beyond.20 A 2023 analysis showed that complex work involving people, which executive roles are full of, was specifically linked to better memory and greater brain reserve in older adults.21 The protection seems to come from the specific type of cognitive demand required: making strategic decisions, mentoring others, mediating conflicts, and leading complex teams.21 The complex intellectual work that defines executive roles is itself one of the strongest documented protective factors for your aging brain. The years you have spent building professional judgment have also been building cognitive reserve.
It is also worth naming what remains intact through perimenopause. Your accumulated expertise, known as crystallized intelligence, is preserved. Your pattern recognition and professional judgment are not impaired, and your strategic thinking and social awareness continue to function effectively. While the cognitive lapses are real, they occur on top of a solid professional foundation that you have spent decades building.
The interventions that work for perimenopause at work cluster around four areas: sleep, exercise, nutrition, and stress regulation. Hormone therapy is a separate decision that you should discuss with a menopause-trained doctor.
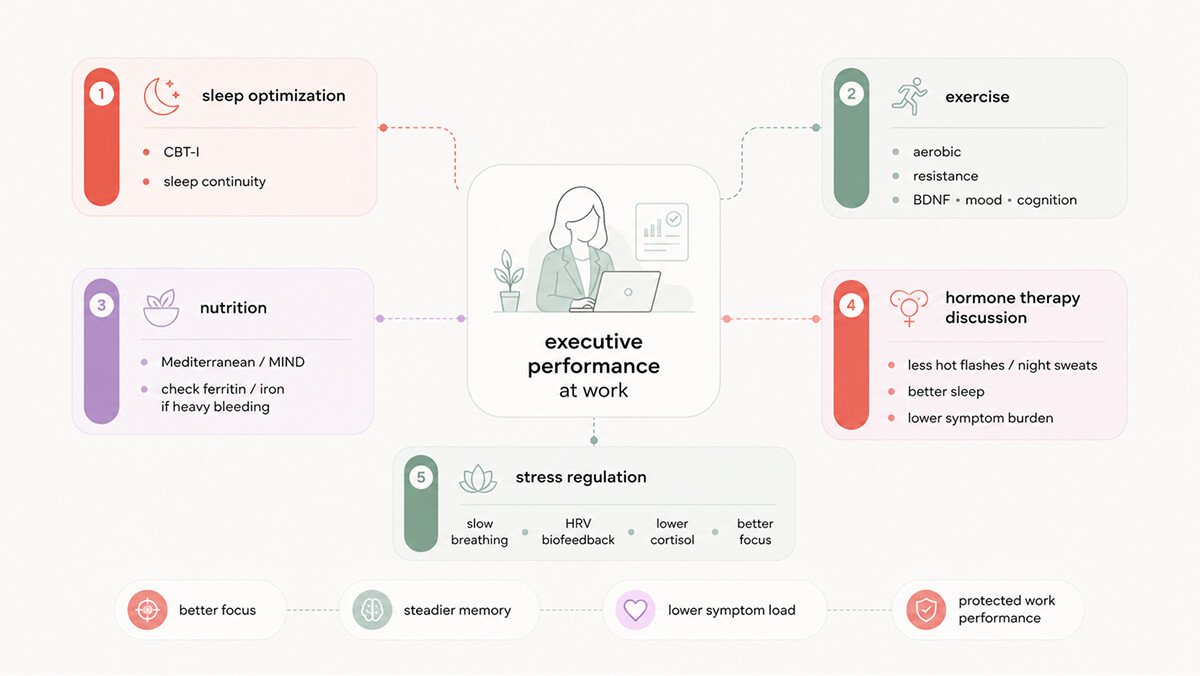

Sleep is the biggest driver of cognitive symptoms during perimenopause, and treating it usually delivers the fastest improvement at work.18 Cognitive Behavioral Therapy for Insomnia (CBT-I) has the strongest evidence base. In one study of perimenopausal and postmenopausal women with insomnia and hot flashes, CBT-I reduced insomnia severity nearly twice as much as menopause education over eight weeks, and the benefits held at six months.22 When researchers pooled results from four large trials, CBT-I outperformed exercise, yoga, omega-3 supplements, and even estradiol for insomnia in menopausal women.23 In postmenopausal women with chronic insomnia, CBT-I also improved work productivity, energy, and emotional well-being.24
The single most reliable thing you can do for your cognitive function in midlife is regular aerobic exercise combined with resistance training.25,26 Exercise increases Brain-Derived Neurotrophic Factor (BDNF), a protein that helps your neurons survive, form new connections, and even grow new neurons in the hippocampus.25,27 In postmenopausal women, a 12-week leisure-time physical activity program raised BDNF and related neurotrophic factors and improved mood.28 A 2024 randomized trial showed that combined physical and cognitive exercise improved executive function and memory in postmenopausal women, alongside increased BDNF.4
A practical starting target is 150 minutes a week of moderate-to-vigorous aerobic activity, plus two sessions of resistance training. Exercise also reduces hot flashes, improves sleep, and lowers cortisol, which addresses several cognitive drivers at once.
The Mediterranean and MIND diets have the most consistent observational evidence for cognitive protection in midlife. A 2025 meta-analysis of 23 studies found that high adherence to the Mediterranean diet was associated with an 11 to 30% reduction in risk of cognitive impairment, dementia, and Alzheimer’s disease.29 Similarly, an analysis of three large groups found that higher MIND diet scores were associated with a decreased risk of dementia.30
However, results from clinical trials are more complex. One three-year study found no significant difference in cognitive performance between those on the MIND diet and a control group when both groups reduced their calories.³¹ While the observational evidence is strong, the direct cause-and-effect relationship isn’t fully proven. Despite this uncertainty, eating a Mediterranean-style diet, rich in vegetables, legumes, whole grains, fish, olive oil, and berries, remains one of the most reliable nutritional strategies for supporting your brain during midlife.
Iron is another crucial factor that often goes overlooked. Up to a quarter of perimenopausal women experience heavy bleeding, which puts them at high risk for iron deficiency. A French study revealed that higher iron levels during midlife predicted better cognitive performance years later, with the link being especially strong for perimenopausal women.32 If you experience heavy cycles and feel mentally sluggish, asking your doctor for a ferritin test is a simple, high-impact step to take.
Hormone therapy is the most effective treatment for vasomotor symptoms like hot flashes and night sweats. However, neither the FDA nor the EMA approves its use specifically for cognitive issues, and current guidelines do not recommend it for that purpose. When cognitive benefits do occur, they are usually a secondary effect of improving sleep and reducing the overall symptom load that causes brain fog.33
The timing of when you start therapy appears to be crucial, with evidence suggesting the greatest benefits come from starting near the onset of menopause rather than years later. This decision is highly individual and depends on your personal history, risk factors, and goals. It should always be discussed with a doctor specializing in menopause.
Chronic stress increases cortisol, which worsens the impact of estrogen withdrawal on your prefrontal cortex. Techniques like slow-paced breathing and heart rate variability (HRV) biofeedback are proven ways to lower immediate stress and sharpen your focus.34,35 Even a single session of HRV biofeedback has been shown to improve attention and provide short-term boosts to working memory.35,36 Furthermore, a higher resting vagal tone, a measure of your “rest and digest” system tracked through HRV, is consistently linked to better executive function and emotional control.37
The practical application is straightforward: breathe at a rate of about six breaths per minute with long exhales for five to ten minutes. This simple practice activates your parasympathetic nervous system and lowers the cortisol load that has been draining your brain’s resources throughout the day.
Everyday tactics fall into three categories: tools for managing symptoms in the moment, structural changes to safeguard your cognitive bandwidth, and strategies for handling the emotional and professional demands of the transition.
The mid-meeting struggle to find a word is often the most painful symptom. However, techniques from performance psychology and military training offer effective solutions that translate perfectly to this situation.
Practicing slow-paced breathing (inhaling for four seconds and exhaling for six) for just 60 to 90 seconds shifts your nervous system into a calmer state. This reduces cortisol and improves your access to working memory within minutes. Best of all, it is a discreet tool you can use under the table without anyone noticing.
From cognitive psychology, cognitive offloading is a technique that reduces the burden on your working memory by moving information from your head onto a visible surface. Having a structured notes page during a meeting, with your three key points written out, frees your prefrontal cortex from the task of holding that information while you simultaneously listen to others. This doesn’t just compensate for a lapse; it prevents the information from being lost in the first place.
From neurorehabilitation, use word substitution. If you can’t find a specific word, don’t stop to search for it. Instead, use a synonym or a brief description and keep moving; the original word usually returns within seconds. Stopping to search puts more pressure on the same brain circuits that are already struggling, making retrieval even harder. Speaking past the gap keeps your flow steady and gives your brain the extra time it needs.
From sports psychology, use implementation intentions. Instead of just trying to remember a future task, make a specific pre-commitment: “When I open my email after this meeting, I will check the contract.” By linking the action to a specific trigger, your brain treats it like an external memory, which significantly reduces the chance of forgetting.
Schedule cognitively demanding work into morning blocks. Cortisol is naturally higher in the early hours and supports alertness. Protect 90-minute uninterrupted blocks for deep work and put administrative tasks in the afternoon.
Lead with your expertise. Your crystallized intelligence (the strategic knowledge you have built over decades) is intact and often at a career peak. Lean into work that requires depth of judgment rather than rapid novel acquisition. Delegate high-speed information processing during peak symptom periods if you can.
Treat sleep as a performance issue, not a comfort issue. Take nocturnal hot flashes as seriously as anything else that affects your work the next day. A cooling mattress pad, a cool bedroom, breathable bedding, and skipping the late glass of wine that fragments REM sleep all change how you show up the next morning.
The anxiety that arises when symptoms appear at work creates its own cognitive burden. Constant self-monitoring, worrying if you’ll forget a word, if others noticed, or if you are losing your edge, consumes the same brain resources you need for clear thinking. Simply identifying this cycle can help break it. These lapses are temporary, biological in nature, and shared by a significant number of women in senior roles.
It is tempting to step away from complex tasks when you feel less sharp, but reducing your mental workload removes the very stimulation that protects your cognitive reserve. Stay engaged with demanding work. Adjust your supporting structures, but do not pull away from the work itself.
Choosing to disclose your symptoms is a personal decision. In supportive environments, being open can lower stress and provide access to practical help. However, in less supportive workplaces, it can be risky. Surveys show that fewer than 10% of senior women with symptoms receive meaningful help at work.15,16 This lack of support has real consequences, leading to declined promotions, job resignations, and disrupted careers.
Perimenopause at work presents a genuine cognitive challenge that often arrives just as career stakes are highest. The biology is clear: estrogen fuels prefrontal cortex function, and when it declines, your working memory, verbal fluency, and processing speed are affected. These changes are physical and real; they are not “all in your head,” nor do they make you less capable.
The essential reframe is that your brain is reorganizing, not failing. The most effective interventions work together: improving sleep, exercise, nutrition, and stress regulation, combined with practical tactics for high-stakes job aspects. By implementing even one strategy from each area, you can see a noticeable difference in your professional performance within weeks. Menopause at work is a temporary phase, not a permanent verdict.
Dr. Jura Lasas
1.
Maki, P. et al. Cognitive changes during the menopausal transition: a longitudinal study in women with and without HIV (2021). https://doi.org/10.1097/gme.0000000000001725
2.
Metcalf, C. et al. Cognitive Problems in Perimenopause: A Review of Recent Evidence (2023). https://doi.org/10.1007/s11920-023-01447-3
3.
Greendale, G. et al. Effects of the menopause transition and hormone use on cognitive performance in midlife women (2009). https://doi.org/10.1212/wnl.0b013e3181a71193
4.
Keawtep, P. et al. Effects of combined dietary intervention and physical-cognitive exercise on cognitive function and cardiometabolic health of postmenopausal women with obesity: a randomized controlled trial (2024). https://doi.org/10.1186/s12966-024-01580-z
5.
Keenan, P. et al. Prefrontal cortex as the site of estrogen’s effect on cognition (2001). https://doi.org/10.1016/s0306-4530(01)00013-0
6.
Jacobs, E. et al. Estrogen Shapes Dopamine-Dependent Cognitive Processes: Implications for Women’s Health (2011). https://doi.org/10.1523/jneurosci.6394-10.2011
7.
Bendis, P. et al. The impact of estradiol on serotonin, glutamate, and dopamine systems (2024). https://doi.org/10.3389/fnins.2024.1348551
8.
Xing, B. et al. Norepinephrine versus dopamine and their interaction in modulating synaptic function in the prefrontal cortex (2016). https://doi.org/10.1016/j.brainres.2016.01.005
9.
Mosconi, L. et al. In vivo brain estrogen receptor density by neuroendocrine aging and relationships with cognition and symptomatology (2024). https://doi.org/10.1038/s41598-024-62820-7
10.
Karlamangla, A. et al. Evidence for Cognitive Aging in Midlife Women: Study of Women’s Health Across the Nation (2017). https://doi.org/10.1371/journal.pone.0169008
11.
Faubion, S. et al. Impact of Menopause Symptoms on Women in the Workplace (2023). https://doi.org/10.1016/j.mayocp.2023.02.025
12.
O’Neill, M. et al. Impact of menopausal symptoms on work and careers: a cross-sectional study (2023). https://doi.org/10.1093/occmed/kqad078
13.
Tserotas, K. et al. Association of menopausal symptoms on work performance in midlife Latin American women (2025). https://doi.org/10.1097/gme.0000000000002645
14.
Clevis, M. et al. Are health-related, lifestyle, work-related, and socio-demographic factors associated with work productivity among menopausal women? A systematic review (2025). https://doi.org/10.1016/j.maturitas.2025.108646
15.
Mallen, S. et al. “I did not recognize myself”: a mixed methods study to better understand the experiences of menopause in a US workplace (2025). https://doi.org/10.1097/gme.0000000000002575
16.
Alzueta, E. et al. Navigating menopause at work: a preliminary study about challenges and support systems (2024). https://doi.org/10.1097/gme.0000000000002333
17.
Safwan, N. et al. Menopause in the workplace: Challenges, impact, and next steps (2024). https://doi.org/10.1016/j.maturitas.2024.107983
18.
Baker, F. et al. Sleep problems during the menopausal transition: prevalence, impact, and management challenges (2018). https://doi.org/10.2147/nss.s125807
19.
Weber, M. et al. Cognitive profiles in perimenopause: hormonal and menopausal symptom correlates (2021). https://doi.org/10.1080/13697137.2021.1892626
20.
Yang, W. et al. Association of Cognitive Reserve Indicator with Cognitive Decline and Structural Brain Differences in Middle and Older Age: Findings from the UK Biobank (2024). https://doi.org/10.14283/jpad.2024.54 /
21.
Coleman, M. et al. Social enrichment on the job: Complex work with people improves episodic memory, promotes brain reserve, and reduces the risk of dementia (2023). https://doi.org/10.1002/alz.13035
22.
McCurry, S. et al. Telephone-Based Cognitive Behavioral Therapy for Insomnia in Perimenopausal and Postmenopausal Women With Vasomotor Symptoms: A MsFLASH Randomized Clinical Trial (2016). https://doi.org/10.1001/jamainternmed.2016.1795
23.
Guthrie, K. et al. Effects of Pharmacologic and Nonpharmacologic Interventions on Insomnia Symptoms and Self-reported Sleep Quality in Women With Hot Flashes: A Pooled Analysis of Individual Participant Data From Four MsFLASH Trials (2017). https://doi.org/10.1093/sleep/zsx190
24.
Kalmbach, D. et al. Improving Daytime Functioning, Work Performance, and Quality of Life in Postmenopausal Women With Insomnia: Comparing Cognitive Behavioral Therapy for Insomnia, Sleep Restriction Therapy, and Sleep Hygiene Education (2019). https://doi.org/10.5664/jcsm.7882
25.
Walsh, E. et al. Towards an understanding of the physical activity-BDNF-cognition triumvirate: a review of associations and dosage (2020). https://doi.org/10.1016/j.arr.2020.101044
26.
Farrukh, S. et al. Association of exercise, brain-derived neurotrophic factor, and cognition among older women: A systematic review and meta-analysis (2023). https://doi.org/10.1016/j.archger.2023.105068
27.
Vedovelli, K. et al. Multimodal physical activity increases brain-derived neurotrophic factor levels and improves cognition in institutionalized older women (2017). https://doi.org/10.1007/s11357-017-9987-5
28.
Kim, B. et al. Regular Leisure-Time Physical Activity is Effective in Boosting Neurotrophic Factors and Alleviating Menopause Symptoms (2020). https://doi.org/10.3390/ijerph17228624
29.
Fekete, M. et al. The role of the Mediterranean diet in reducing the risk of cognitive impairment, dementia, and Alzheimer’s disease: a meta-analysis (2025). https://doi.org/10.1007/s11357-024-01488-3
30.
Chen, H. et al. Association of the Mediterranean Dietary Approaches to Stop Hypertension Intervention for Neurodegenerative Delay (MIND) Diet With the Risk of Dementia (2023). https://doi.org/10.1001/jamapsychiatry.2023.0800
31.
Barnes, L. et al. Trial of the MIND Diet for Prevention of Cognitive Decline in Older Persons (2023). https://doi.org/10.1056/nejmoa2302368
32.
Andreeva, V. et al. Midlife iron status is inversely associated with subsequent cognitive performance, particularly in perimenopausal women (2013). https://doi.org/10.3945/jn.113.177089
33.
Joffe, H. et al. Estrogen therapy selectively enhances prefrontal cognitive processes: a randomized, double-blind, placebo-controlled study with functional magnetic resonance imaging in perimenopausal and recently postmenopausal women (2006). https://doi.org/10.1097/01.gme.0000189618.48774.7b
34.
Sévoz-Couche, C. et al. Heart rate variability and slow-paced breathing: when coherence meets resonance (2022). https://doi.org/10.1016/j.neubiorev.2022.104576
35.
Blaser, B. et al. The effect of a single-session heart rate variability biofeedback on attentional control: does stress matter? (2023). https://doi.org/10.3389/fpsyg.2023.1292983
36.
Bahameish, M. et al. Short-Term Effects of Heart Rate Variability Biofeedback on Working Memory (2024). https://doi.org/10.1007/s10484-024-09624-7
37.
Forte, G. et al. The intricate brain-heart connection: The relationship between heart rate variability and cognitive functioning (2024). https://doi.org/10.1016/j.neuroscience.2024.12.004

Mood & Energy Solutions

Fatigue Causes & Types
Fatigue Causes & Types

Workplace Strategies

Menopause at Work

Brain Fog at Work

Brain Fog at Work

Is This Perimenopause?

Is This Perimenopause?

Nutrition & Supplements

Workplace Strategies

Menopause Science

Menopause Science

Brain Fog Solutions
We use cookies and similar technologies to ensure the proper functioning of our website, personalize content, provide social media features, and analyze traffic. By clicking “I Agree”, you consent to the use of these technologies.
No results




