22 June 2026
Why Menopause Stress and Anxiety Feel Harder to Manage

Reading time 11 min.

Reading time 11 min.
You used to absorb pressure. Work deadlines, difficult conversations, competing priorities – your nervous system handled it, recovered, and moved on. You can still absorb a missed deadline or a hard review. The small ones have started to register differently: a silly comment in a meeting, someone’s chit-chat in the coffee line, ordinary friction that once passed without notice.
Your reactions feel disproportionate. The gap is widening between the person you know yourself to be and how you are actually responding. Menopause stress and anxiety often begin here, in small escalations over ordinary moments. Most women notice only after the pattern is already set.
The change in menopause stress tolerance doesn’t signal that you are losing your edge. It’s a measurable neurobiological change. During perimenopause, multiple stress-regulating systems begin changing at once. The brain becomes quicker to register threats. The neurochemical systems that help you calm down lose estrogen support. The prefrontal cortex (the region that keeps you composed under pressure) loses support. And the autonomic nervous system becomes prone to chronic overdrive.
Together these systems explain why perimenopause stress sensitivity is so visceral and why understanding the specific mechanisms matters for choosing interventions that actually work.
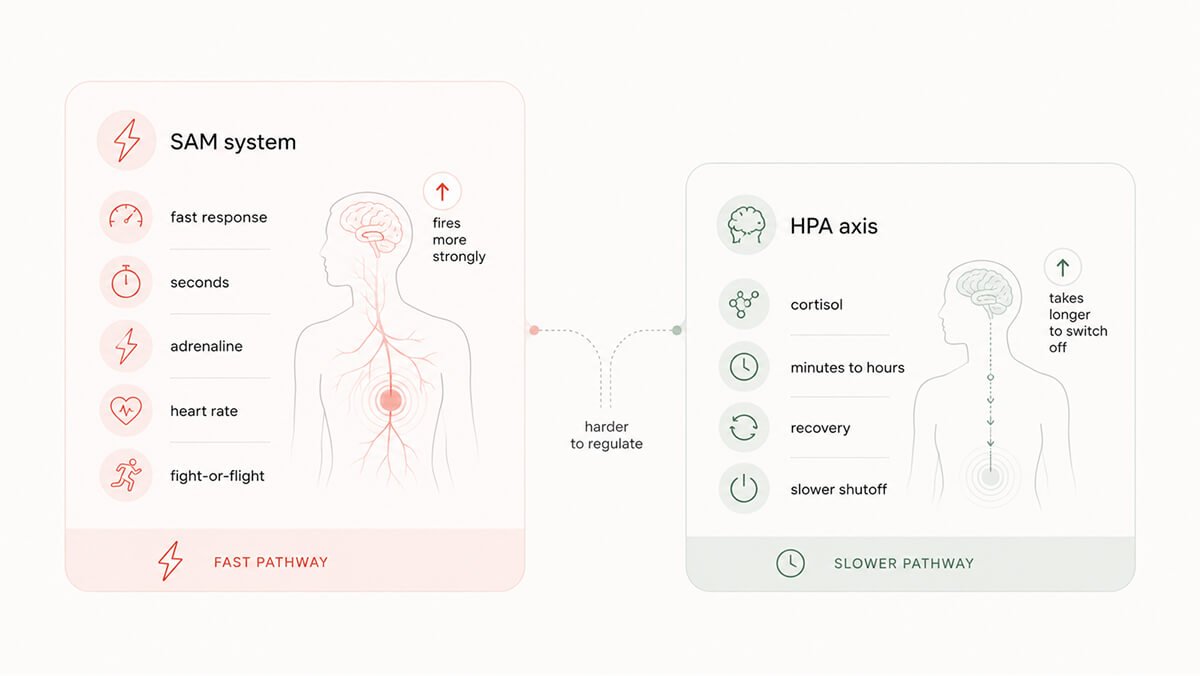
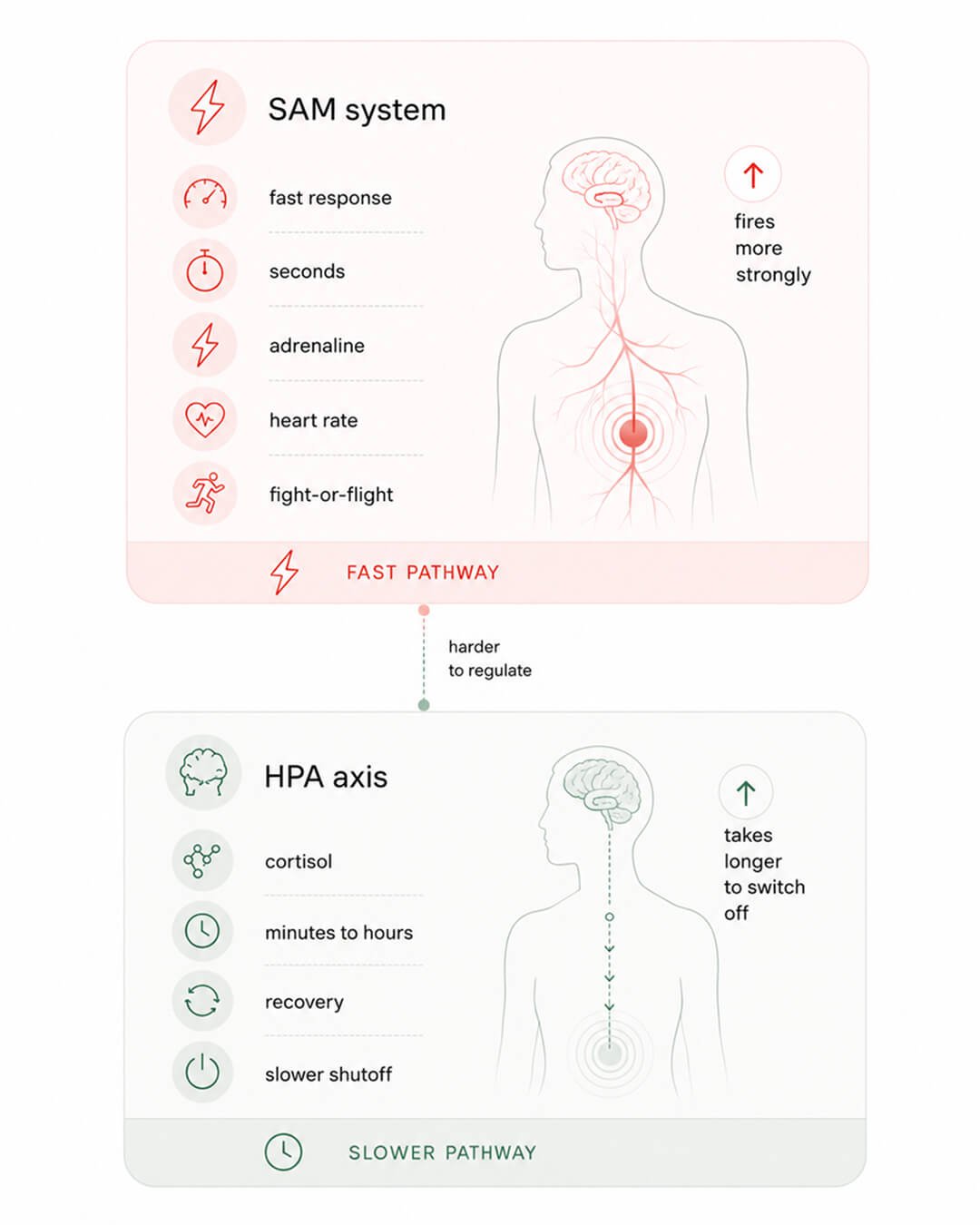
You have two stress systems and perimenopause affects them both.1 This is why menopause stress and perimenopause stress feel different from what you knew earlier in life.
The first is fast. The sympathetic-adreno-medullary (SAM) system is a near-immediate neural response: within seconds of a stressor, it floods your system with adrenaline and norepinephrine, which drive up your heart rate, blood pressure, and blood flow to muscles. This is the immediate fight-or-flight surge, and in perimenopause stress it fires harder and faster than it used to. It’s what you feel in your chest when someone blindsides you in a meeting (or if you get attacked by an animal).
The second is slower. The hypothalamic-pituitary-adrenal (HPA) axis is hormonal: the hypothalamus signals the pituitary, which signals the adrenals to release cortisol. Cortisol helps sustain the stress response for minutes to hours. Cortisol helps mobilize energy, modulate immune function and support recovery. When the stressor passes, cortisol feeds back to the hypothalamus and hippocampus to shut the loop down. The system is designed to be self-limiting. Fire, respond, recover. In perimenopause, the recover step stops working reliably, and menopause anxiety often begins here.
These two systems co-activate but serve different functions: SAM handles survival-speed demands (think tiger or CFO attacks), while the HPA axis manages your recovery and helps shut down that initial stress surge once the danger has passed. In a well-regulated system, they work as partners. During perimenopause, both are impaired at the same time. Menopause stress becomes harder to regulate because the partnership itself has broken down.
Estrogen acts like a dimmer switch on your cardiovascular stress response. Before menopause, estrogen helps blood vessels stay more relaxed and less reactive to adrenaline, providing a protective offset. When your sympathetic nerves fire in response to stress, your blood pressure can still rise, but estrogen blunts how big and how fast that spike tends to be. However, once estrogen levels drop after menopause, this protective offset is largely lost. Now, the same stress signal causes blood vessels to tighten faster, leading to higher vascular resistance and blood pressure.2
Studies show that postmenopausal women, even when resting, have a sympathetic nerve firing rate nearly three times higher than younger women. When faced with a stress challenge like exercise, their response is more than doubled, resulting in a much larger jump in blood pressure.3 Research agrees that menopause shifts the heart’s automatic control towards sympathetic dominance, meaning the “gas pedal” is pressed harder than the “brake”. The imbalance is what menopause anxiety actually feels like physically: the body stays accelerated long after the stressor has passed.
The jittery, wired feeling after a stressful moment, say, a tense conversation at 4 p.m., can persist for hours. Your heart rate might stay elevated, your jaw remains clenched, and you may lie in bed at 9 p.m. still physically activated. The calming parasympathetic brake that should return your body to baseline is simply weaker. For healthy postmenopausal women, the “gas pedal” system (sympathetic activity) dominates even at rest, as the natural calming “brake” (vagal predominance) that premenopausal women rely on is no longer in charge.
The disruption to the HPA axis (your slow, recovery system) is equally important. Think of this system as a furnace that heats your home when the temperature drops (stress hits). For the furnace to work properly, it needs a thermostat to turn it off when the room is warm enough (stress has passed).
One crucial component of this thermostat is a neurosteroid called allopregnanolone. This calming chemical is made from progesterone (which drops sharply in perimenopause) and acts like your brain’s natural volume knob for GABA receptors (the same ones targeted by anti-anxiety medications like benzodiazepines). As progesterone levels fall, you lose this internal calming boost. In scientific terms, the HPA axis becomes “sensitized,” meaning your body’s cortisol response escalates and is much less efficient at shutting itself down.1
The brain’s control center for the feedback process in both stress systems is the hippocampus. The hippocampus is highly sensitive to estrogen and is responsible for two vital jobs: first, helping distinguish a real threat from a perceived one, and second, sending the final “all-clear” signal to turn off the cortisol release.
When estrogen declines, the hippocampus loses its hormonal protection and its ability to shut off the stress response weakens. Less estrogen means less inhibitory feedback from the hippocampus, which leaves more cortisol in circulation. Over time, chronically high cortisol damages the hippocampus itself. Hippocampal weakening and rising cortisol reinforce each other, and perimenopause stress becomes self-sustaining: constant in the body, harder to escape from the inside.4
Curious fact: Allopregnanolone is so central to brain and mood regulation that an intravenous formulation of it (brexanolone) became the first FDA‑approved drug specifically for postpartum depression. The same neurosteroid GABA pathway that swings abruptly after childbirth also changes during perimenopause, likely contributing to mood vulnerability, yet this connection is rarely discussed with patients in most clinical settings.5
If the two stress systems are the accelerators, the prefrontal cortex (PFC) is the brake. The PFC handles executive function: cognitive flexibility, impulse control, the capacity to override a reactive amygdala response with measured judgment. In a board meeting where someone challenges your data, the PFC is what keeps you responding strategically instead of defensively. It’s the infrastructure behind emotional regulation that menopause depletes.
Estrogen is not a peripheral reproductive hormone that incidentally touches the brain. It’s an active neuromodulator with receptors distributed throughout the PFC, amygdala, hippocampus, and brainstem, acting on multiple neurotransmitter systems simultaneously. Estrogen boosts serotonin synthesis, so when estrogen declines, lowered serotonin levels decrease mood stability and make you more prone to depressive reactions when facing stress. Estrogen also modulates dopamine neuron activity, influencing reward processing and motivation. Finally, it also restrains norepinephrine reactivity, and without estrogen’s moderating influence, the hypervigilance and anxiety can spike. Each of these systems destabilizes together.
Under normal hormonal conditions, the PFC exercises top-down control over the amygdala – your brain’s threat-detection center. The PFC evaluates, contextualizes, and when appropriate, overrides the amygdala’s alarm signal. That override depends on adequate glutamate signaling and number of neuronal connections in the PFC, both of which estrogen supports.6
Neuroimaging studies show when estrogen declines, the amygdala seems to activate more often, establishing an intense, “hyperconnected” link with the medial PFC. This is a pattern frequently seen in depression, reflecting an amygdala that remains tonically activated without adequate top-down regulation from the PFC. Interestingly, one study found that just three weeks of transdermal estradiol helped quiet this overactive circuit, decreasing the hyperconnectivity alongside symptom improvement.7
Why does the prefrontal “brake” weaken? Estrogen supports the critical chemical signals necessary for PFC function, especially glutamate and GABA. Separate research shows that perimenopausal women have lower levels of these vital neurotransmitters in the PFC compared to premenopausal women, offering a plausible neurochemical basis for the loss of emotional control. While these are small, early studies establishing a mechanism, the findings are consistent, and the underlying biology makes sense.
The challenges run deeper than just neurotransmitter levels; they involve the brain’s energy supply. Landmark neuroimaging research from Lisa Mosconi and her team has shown that during the menopausal transition, the brain’s raw fuel glucose is significantly depleted. Using PET imaging, their 2021 study revealed that middle-aged women experienced up to a 30% drop in brain glucose metabolism compared to their premenopausal baseline, a deficit not seen in age-matched men.8 This metabolic slowdown was concentrated in areas responsible for emotional control and higher-order thinking, confirming it is an effect of menopause, not just getting older. A 2024 follow-up study provided another crucial piece of the puzzle: as estrogen declines, the brain’s frontal cortex and hippocampus try to compensate by growing more estrogen receptors, desperately attempting to capture the remaining hormone. Unfortunately, this increase in receptor density was found to correlate with more severe mood symptoms and poorer performance on cognitive tests.9
That familiar, visceral reaction to a small work annoyance, like the rage when a colleague misses a deadline or the sharp retort when someone takes credit for your idea, isn’t a personality flaw. It’s your brain’s CEO, the PFC, trying to manage an executive crisis with a cut budget. The PFC, which handles composure and strategic judgment, is suddenly running on critically low neurochemical fuel. Your brain is struggling with a genuine, measurable neurochemical deficit in the region responsible for keeping you composed. This is the reality of perimenopause stress tolerance in the professional context.
Sleep disruption during perimenopause is not a minor inconvenience stacked on top of the real problems. Based on emerging experimental evidence, sleep disruption is a primary driver of HPA axis dysfunction and potentially more consequential than the hormonal changes themselves.
A 2023 Yale study specifically separated the effects of sleep loss from estrogen decline. The results were striking: while low estrogen set the stage, it was the fragmented sleep that threw the HPA axis into disarray. Sleep loss significantly elevated bedtime cortisol and blunted the essential morning cortisol response. Without sleep problems, estrogen suppression by itself did not cause these major cortisol changes.10 For perimenopause stress, sleep is the lever: fix sleep and cortisol will follow.
An estimated 40–60% of menopausal women struggle with sleep disturbances coming down to key hormonal shifts:
I know what it feels like to feel a surge of irritation so sharp it scares you. Not because of what happened, but because of how wildly your reaction exceeded the situation. And then to wonder if something is genuinely wrong with you.
Nothing is wrong with you. Your menopause stress tolerance changed because multiple neurobiological systems shifted simultaneously.
Two stress axes lost their hormonal regulation, the prefrontal cortex lost its neurochemical fuel, sleep disruption drove cortisol into a self-reinforcing loop, and the brain’s energy supply to the regions responsible for composure measurably dropped. The brain is remodeling, not declining.
Dr. Jura Lasas
1.
Hantsoo, L. et al. The role of the hypothalamic–pituitary–adrenal axis in depression across the female reproductive lifecycle: current knowledge and future directions (2023) https://doi.org/10.3389/fendo.2023.1295261
2.
Klassen, S. A. et al. The impact of ageing and sex on sympathetic neurocirculatory regulation (2021) https://doi.org/10.1016/j.semcdb.2021.01.001
3.
Wenner, M. M. et al. Influence of Age and Estradiol on Sympathetic Nerve Activity Responses to Exercise in Women (2022) https://doi.org/10.1249/MSS.0000000000002823
4.
De Nicola, A. F. et al. Estrogens and Neuroendocrine Hypothalamic–Pituitary–Adrenal Axis Function (2006) https://doi.org/10.1159/000094324
5.
McEvoy, K. et al. Allopregnanolone and reproductive psychiatry: an overview (2019) https://doi.org/10.1080/09540261.2018.1553775
6.
Yap, S. et al. Decreased Medial Prefrontal Cortex Glutamate Levels in Perimenopausal Women (2021) https://doi.org/10.3389/fpsyt.2021.763562
7.
Hynd, M. et al. Estradiol modulates resting-state connectivity in perimenopausal depression (2024) https://doi.org/10.1016/j.jad.2024.11.068
8.
Mosconi, L. et al. Menopause impacts human brain structure, connectivity, energy metabolism, and amyloid-beta deposition (2021) https://doi.org/10.1038/s41598-021-90084-y
9.
Mosconi, L. et al. In vivo brain estrogen receptor density by neuroendocrine aging and relationships with cognition and symptomatology (2024) https://doi.org/10.1038/s41598-024-62820-7
10.
Cohn, A. Y. et al. Effects of Sleep Fragmentation and Estradiol Decline on Cortisol in a Human Experimental Model of Menopause (2023) https://doi.org/10.1210/clinem/dgad285

Mood & Energy Solutions

Fatigue Causes & Types
Fatigue Causes & Types

Workplace Strategies
Menopause at Work

Brain Fog at Work

Brain Fog at Work

Is This Perimenopause?

Is This Perimenopause?

Nutrition & Supplements

Workplace Strategies

Menopause Science

Menopause Science

Brain Fog Solutions
We use cookies and similar technologies to ensure the proper functioning of our website, personalize content, provide social media features, and analyze traffic. By clicking “I Agree”, you consent to the use of these technologies.
No results





