22 June 2026
Wired, Exhausted, and Anxious? The Perimenopause Nervous System Explained

Reading time 16 min.

Reading time 16 min.
You went to bed at a reasonable hour. You did everything right. You woke up at 3am with your heart pounding and your mind running, and you could not fall asleep again. By 9am you were bone-tired and somehow buzzing. By 11am, anxious for no obvious reason. The perimenopause nervous system feels like it’s in a conflict with itself. Wired, exhausted, anxious, all at once. The temptation is to read these as three different problems. However, they share the same mechanisms and can be understood as if they were one.
The biggest mistake most people make is treating perimenopause as estrogen “dropping.” The drop is not what destabilizes your nervous system. The instability does. Estrogen in perimenopause moves in unpredictable swings, sometimes higher than in your reproductive years, sometimes near zero, week to week. Progesterone falls earlier and more steadily. Your brain is built to read these hormones like a thermostat. It is not well equipped to react to chaos.1
Estrogen is a master neuromodulator. Estrogen isn’t the “message” in the brain itself; it’s the volume control that determines how strongly your brain cells communicate. Its receptors are not found only in your ovaries. They are scattered through the brain, in every region that handles stress, mood, attention, body temperature, and sleep. The brain area hypothalamus runs your stress response and your thermostat. The hippocampus is where memory and stress regulation meet. The amygdala (your brain’s alarm center) reads threats. The locus coeruleus floods you with norepinephrine when something feels urgent. The raphe nucleus makes most of your serotonin. Every one of these regions has estrogen receptors and uses estrogen to keep its work running smoothly.2,3
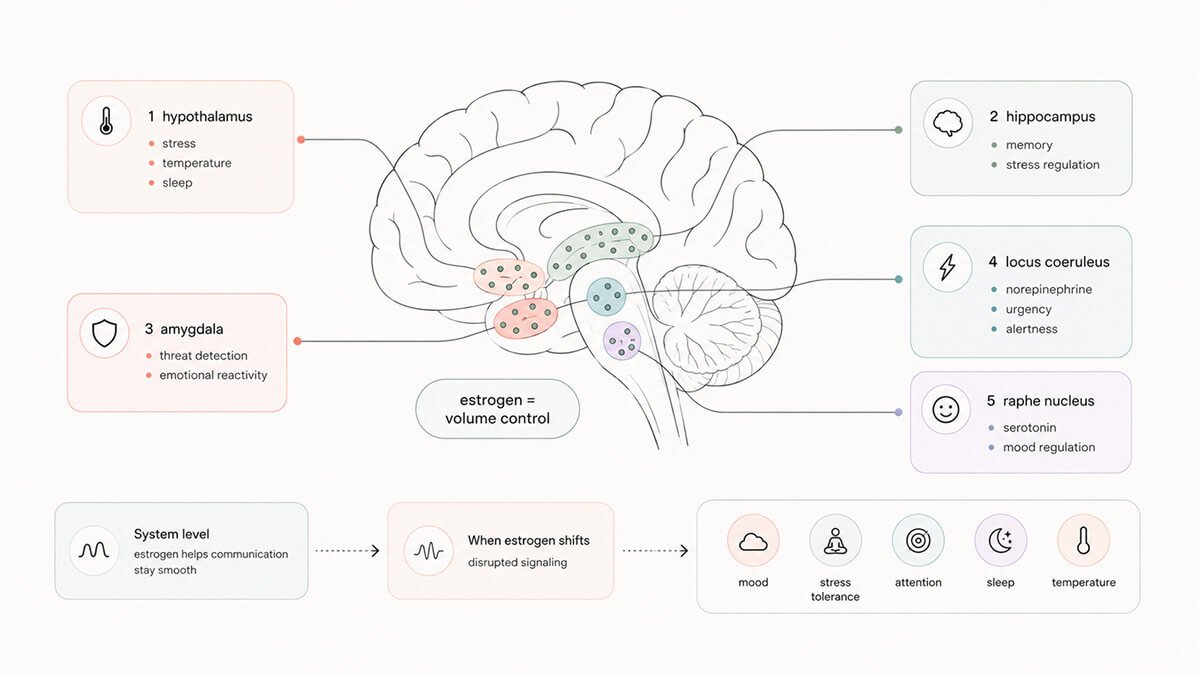
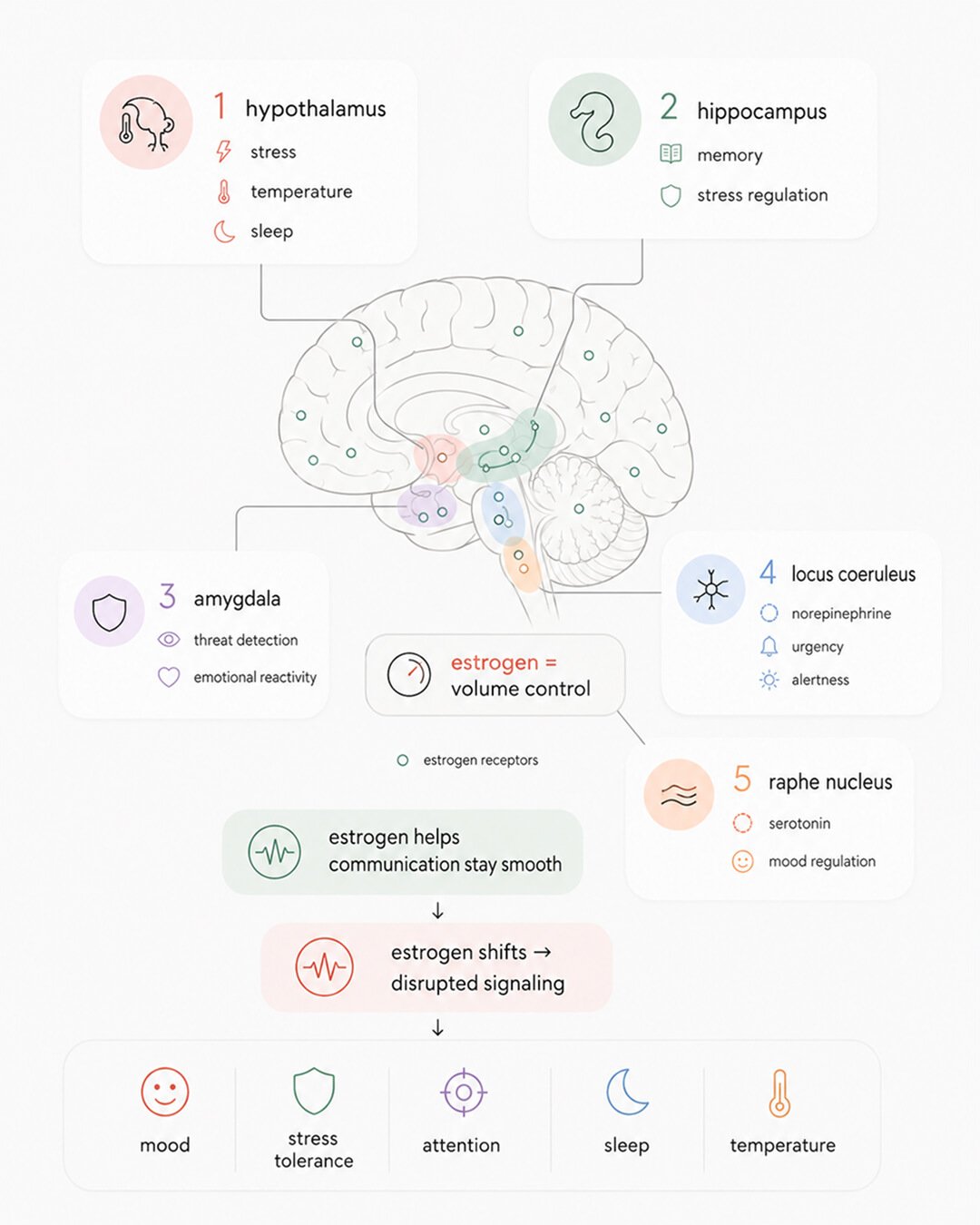
When estrogen is stable, you do not notice anything unusual. Your nervous system runs in the background, balanced and self-correcting. When estrogen starts to fluctuate unpredictably, every one of these regions starts to misfire on its own timeline. Some weeks the alarm center is too loud. Other weeks the serotonin supply runs short. Some mornings the stress system cannot shut itself off. You feel such brain behaviors as random anxiety, random tearfulness, random sleeplessness, and random “wired but tired” days. It might look and feel random to you. From the brain’s perspective, it is the predictable result of a master regulator losing its rhythm.
Progesterone matters here in a way most women have never been told. In your brain, progesterone is converted into a compound called allopregnanolone. Allopregnanolone is your brain’s natural anti-anxiety chemical. It works on the same brain receptors (called GABA receptors) that anti-anxiety medications target. When progesterone falls and stays low, your brain loses its built-in calming signal at exactly the moment estrogen volatility is dialing up the alarm.4 The combination is what makes perimenopause anxiety feel sharper and harder to talk yourself out of than anything you remember.
Curious Fact. The strongest predictor of who develops perimenopause anxiety is not how low estrogen falls. It is how much it fluctuates from week to week. A 2022 randomized clinical trial found that women who were most sensitive to estrogen swings before treatment responded best to a transdermal estrogen patch that stabilized those swings. The patch addressed the instability, and the anxiety improved with it.5
Everything that follows in this article is downstream of estrogen instability. Five other systems are affected because the master regulator above them is no longer steady.
Your slow stress system is called the HPA axis: hypothalamus to pituitary to adrenal glands. When something stressful happens, your hypothalamus signals down the chain, and your adrenal glands release cortisol. Cortisol keeps you alert and mobilized for minutes to hours. When the stressor passes, rising cortisol is supposed to feed back upstream and switch the cascade off. That feedback loop is what keeps a normal stress response from running forever. In perimenopause, the off-switch stops working reliably.6
Estrogen and progesterone both help that off-switch function. Estrogen sensitizes the brain regions that receive the “all clear” cortisol signal. Progesterone, through allopregnanolone, dampens the alarm system that started the cascade in the first place. When both hormones go unstable, you lose pressure on the brake at the moment something is pressing harder on the gas. Cortisol stays high longer. Recovery slows. The next stressor lands on a system that has not fully reset from the last one. This is how the menopause nervous system tips into chronic low-grade activation.7
In clinical research, the low-grade activation looks like specific cortisol patterns. Some women run high cortisol throughout the day. Others have high cortisol at night, especially when sleep is broken (the classic “wired at 3am, exhausted at 9am” picture). The third group has a flattened curve, where the normal morning peak that helps you wake up disappears. All three patterns are linked to worse mood, worse sleep, and slower recovery from ordinary daily friction.8
The 2022 randomized clinical trial mentioned in the previous section gives the clearest evidence that variability is the real driver here. Women whose baseline cortisol responses were most reactive to estrogen fluctuations had the strongest anxiety response, and they also had the strongest improvement when transdermal estrogen smoothed the fluctuations.5 The HPA axis is not broken in some women but intact in others. It is more or less sensitive to the upstream estrogen chaos. The same estrogen chaos creates very different downstream pictures for different women depending on their baseline reactivity.
For many women, the experience is that small things feel disproportionate. A short email lands like a confrontation. A delayed train turns the morning into a disaster. You used to absorb these without noticing, and now your brain stays activated for hours. That extended activation is the inability to recover from the HPA axis activation. The mechanism is biological, and the pattern keeps repeating because the estrogen dampener is going away.
Estrogen shapes the supply, the release, and the sensitivity of three of your brain’s most important neurotransmitters. As estrogen becomes unstable, all three start to falter at once, on slightly different timelines, in slightly different regions. What you feel is the sum of those simultaneous changes.
Serotonin is what most women have heard of, because it is what most antidepressants act on. Estrogen helps your brain produce serotonin and also helps your brain use it. When estrogen falls and fluctuates, serotonin signaling weakens. Mood becomes less stable. Your tolerance for friction shrinks, and small irritations turn into major events. This is one mechanism behind both perimenopause anxiety, the irritability and tearfulness that often come months before any obvious mood diagnosis.9
Dopamine controls motivation, focus, and the small daily payoff that makes you want to start tasks. As estrogen fluctuates, your brain produces less dopamine and responds less to it. The result feels like wading through mud. You used to push through to write the report. Now starting it feels like rolling a boulder uphill. This is one of the mechanisms behind the exhausted mornings women describe when they are sleeping enough but cannot get motivation.10
GABA is your brain’s main “off switch.” It is what keeps your brain cells from firing too much, too easily, for too long. Estrogen and progesterone (through allopregnanolone) both support GABA signaling. One small study used magnetic resonance spectroscopy to look at GABA levels in the anterior cingulate cortex of perimenopausal women with depression. They found GABA levels were significantly lower than in healthy controls.¹¹ Less GABA means your brain cells are activated more easily and stay active longer, because the chemical that normally tells them to settle is no longer there in the right amounts. From the inside, this feels like a body that will not calm down, a mind that will not stop, and a startle response triggered by the events that did not used to bother you.
These three neurotransmitters do not change one by one in a tidy order. They wobble together. That is why anxiety, exhaustion, irritability, and low motivation tend to arrive in clusters, not one at a time. A single week can bring all four. Women often describe this as “I do not recognize myself.” From the neurochemistry side, recognition is exactly what you would expect to lose when three independent regulatory systems all start to drift at once.
This is the part of the perimenopause nervous system story that most women have never been told.
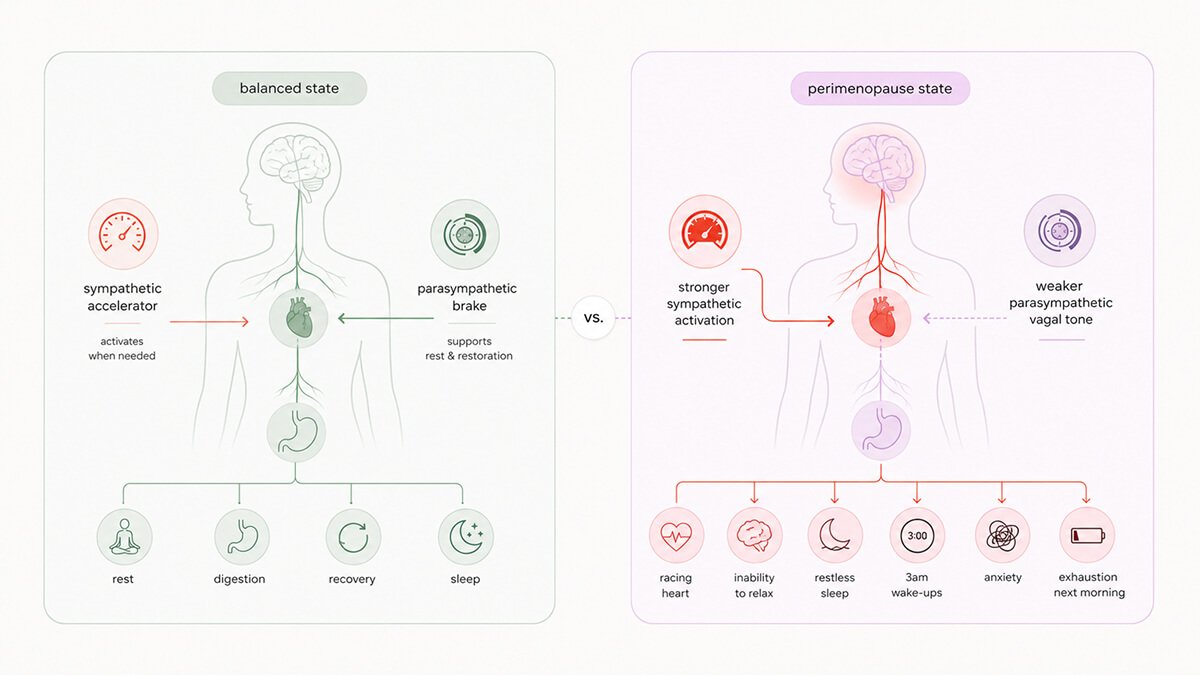
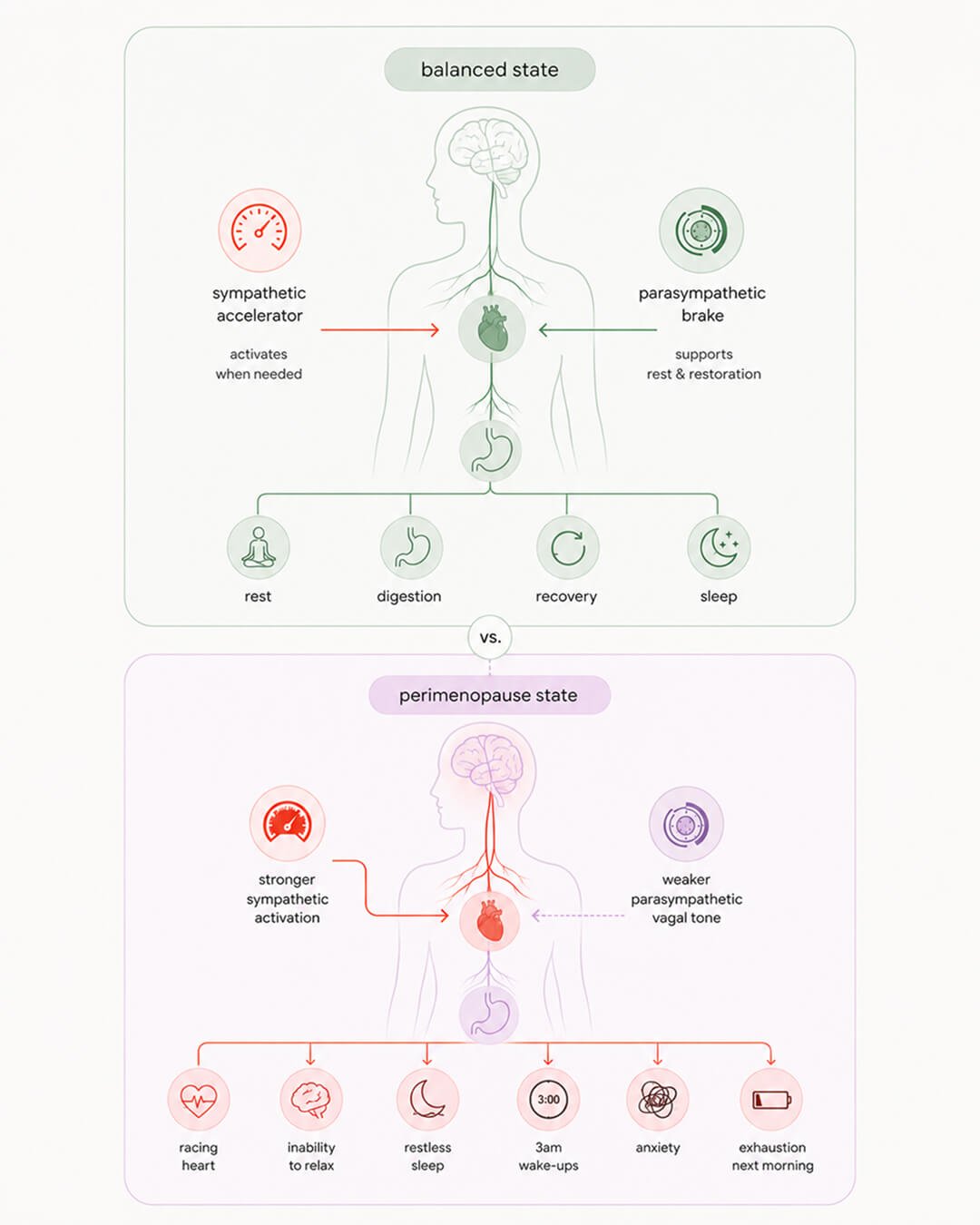
Your autonomic nervous system has two halves. The sympathetic half is your accelerator: heart rate up, blood pressure up, alertness up, ready to react. The parasympathetic half is your brake: heart rate down, digestion on, recovery happening, body settling. In a healthy nervous system, the brake is dominant most of the time. The accelerator engages when needed and then disengages. The brake stays in the background, doing the quiet work of recovery.12
In perimenopause, that balance flips. The accelerator runs more often, harder, and longer. The brake (your vagal tone) weakens. This is the mechanism most directly responsible for “wired but tired.” When your sympathetic system is dominant and your parasympathetic recovery is muted, your body cannot down-regulate, even when there is nothing to react to. You feel activated. You feel exhausted. Both at the same time. This is what an autonomic nervous system without a working brake will produce.
Researchers have measured this directly in women. In a series of studies on perimenopausal women with insomnia, scientists tracked heart rate, heart rate variability (HRV), and EEG activity during sleep. The women with insomnia showed elevated heart rates and reduced vagal tone even during the periods of sleep when nothing was waking them up. Their bodies were running sympathetic tone through the night.¹³ This is the autonomic nervous system in the wrong gear during the hours that should be recovery.
Curious Fact. Women with menopausal insomnia have elevated heart rate and reduced vagal tone during undisturbed sleep. The body is running in fight-or-flight even when nothing is wrong. You wake up tired because your nervous system has been working all night.
Estrogen supports vagal tone directly. It helps the parasympathetic system stay strong and responsive. As estrogen becomes unstable, the brake weakens, and the sympathetic accelerator faces less resistance. Sleep loss makes it worse. So does cortisol that has not come down from yesterday. So does an extra coffee, a hard meeting, a difficult conversation, or a bad piece of news. Each of these inputs reinforces the others. The system tips, and once it tips, it stays tipped without deliberate intervention.14
This is the layer that explains why so many women describe perimenopause as feeling “switched on.” The constant low-grade alertness comes from autonomic dominance without a counterweight. It is also the layer most amenable to intervention. Slow breathing, paced at around six breaths per minute, directly stimulates the vagus nerve and brings the brake back online. Cold water exposure, certain forms of meditation, and steady aerobic movement do the same thing on different timelines.
There is a layer of perimenopause biology that underlies everything else. Your brain runs on glucose and cannot store fuel. It needs every system feeding it to keep working in real time without any breaks. It is the most metabolically expensive organ in your body, and it has no margin for interruption.
Estrogen is central to brain energy. It supports glucose uptake in brain cells, supports mitochondrial function (the cellular machinery that turns glucose into usable energy), and keeps the brain’s resident immune cells (microglia) in a calm, protective state. When estrogen becomes unstable, all three layers are disrupted at once. Brain energy production drops. Inflammation rises. The energy-producing machinery itself starts to falter.15,16
In landmark neuroimaging work by Lisa Mosconi, midlife women show measurable reductions of up to 30% in brain glucose metabolism in the same regions affected by perimenopause symptoms: the prefrontal cortex, the hippocampus, and the anterior cingulate. Age-matched men do not show this pattern. The signal is hormonal, not chronological.17
Dr. Roberta Brinton has described perimenopause as a “neurological transition state,” and the framing is precise. Your brain is not aging on a normal curve. It is going through a metabolic restructuring that can either resolve into a new stable state or continue to lose ground. For most women brain restructuring resolves. But for some it does not. The ones who do not are at higher risk for later neurodegenerative disease, which is one reason this transition matters far beyond symptom management.15
At the same time, microglia become pro-inflammatory in the regions most central to mood and stress regulation. One major review framed perimenopause as a systemic inflammatory phase, with consequences that extend from menopause symptoms into later disease risk.18 When inflammation in the brain is high, brain cells neurons communicate less efficiently and do not recover well from ordinary stress. The mood symptoms, the brain fog, the sleep fragmentation, and the fatigue all connect to this inflammatory layer.
Impaired glucose metabolism and neuroinflamation are why exhaustion in perimenopause does not respond to a good night’s sleep the way it used to. The fatigue is not a sleep debt that one weekend can fix. The problem is energy production at the cellular level, faltering across the regions of the brain you most rely on for complex thought, emotional regulation, and memory. The menopause nervous system needs the mechanism addressed, not just the symptom.
Sleep is where every system above either repairs or breaks down further. In perimenopause, sleep often is disrupted. Around 40 to 60% of perimenopausal women report sleep disturbance. The classic picture is falling asleep fine and then waking at 3 or 4am, wired and anxious, unable to fall back asleep. This is the autonomic nervous system and HPA axis story we discussed above, playing out at night.19
Nighttime hot flashes are one driver. The hypothalamus runs your body’s thermostat, and estrogen helps it set a stable temperature. When estrogen fluctuates, the thermostat misreads tiny temperature changes as emergencies and triggers sudden, intense bursts of heat to cool the body down at the wrong times. The hot flash itself is brief, but the surge of norepinephrine that accompanies it can keep you awake for an hour. Even when you do not fully wake up, the surge fragments sleep architecture, especially the deep stages that do most of your physical recovery.20
Sleep loss then feeds back into everything else. One night of fragmented sleep raises cortisol the next day. Repeated nights of fragmented sleep blunt the morning cortisol peak you need to feel alert when you wake up. They reduce vagal tone. They worsen inflammation and drop dopamine signaling strength. Bad sleep strains the prefrontal cortex, which then has less capacity to regulate the alarm center. By the time a perimenopausal woman has been through six months of broken sleep, her nervous system is operating from a much weaker baseline than it was six months earlier, even if nothing else has changed.21
The brain itself starts to look different in scans. Neuroimaging in perimenopausal brains has shown altered activity in the prefrontal cortex and the cingulate cortex, the two regions most central to emotional regulation and attention. Lower estrogen levels correlate with higher anxiety scores and with the specific brain activity patterns linked to that anxiety.²² The change is structural and functional.
This is also why one of the highest-leverage interventions in perimenopause is fixing sleep. Cognitive Behavioral Therapy for Insomnia (CBT-I) has the strongest evidence base. Where nighttime hot flashes drive the awakenings, hormone replacement therapy (HRT) is often the most direct fix. Sleep is not a separate problem alongside everything else. It is the layer that determines whether the rest of the system can recover.23
The six mechanisms together are one cascade. Hormonal instability disrupts the master regulator estrogen, which destabilizes everything downstream. The HPA axis, the neurotransmitters, the autonomic balance, the brain’s energy supply, the inflammatory tone, and the sleep that should be repairing all of them. Every downstream system runs off the same upstream estrogen chaos. The wired-and-tired-and-anxious cluster comes from one biology, expressed in three different rooms of your life at the same time.
I’ve been there myself. I know the 3:00 a.m. wake-ups, the anxiety that appears out of nowhere, and the kind of exhaustion that a weekend of rest can’t fix. During perimenopause, the nervous system undergoes a genuine restructuring. Those “wired” mornings and the persistent perimenopause anxiety, which can sometimes linger for years, all share the same biological root.
Understanding this mechanism doesn’t solve everything overnight, but it does change how you read your own body. You stop fighting your nervous system and start working with your biology.
Dr. Jura Lasas
1.
Fidecicchi, T. et al. Neuroendocrine mechanisms of mood disorders during menopause transition: A narrative review and future perspectives (2024). https://doi.org/10.1016/j.maturitas.2024.108087
2.
Cho, J. et al. Beyond Hot Flashes: The Role of Estrogen Receptors in Menopausal Mental Health and Cognitive Decline (2025). https://doi.org/10.3390/brainsci15091003
3.
Crockett, C. et al. Menopause and Mental Health (2025). https://doi.org/10.1007/s12325-025-03427-w
4.
Bencker, C. et al. Progestagens and progesterone receptor modulation: Effects on the brain, mood, stress, and cognition in females (2024). https://doi.org/10.1016/j.yfrne.2024.101160
5.
Lozza-Fiacco, S. et al. Baseline anxiety-sensitivity to estradiol fluctuations predicts anxiety symptom response to transdermal estradiol treatment in perimenopausal women: A randomized clinical trial (2022). https://doi.org/10.1016/j.psyneuen.2022.105851
6.
Gordon, J. et al. Ovarian hormone fluctuation, neurosteroids, and HPA axis dysregulation in perimenopausal depression: a novel heuristic model (2015). https://doi.org/10.1176/appi.ajp.2014.14070918
7.
Han, Y. et al. Neuroendocrine pathogenesis of perimenopausal depression (2023). https://doi.org/10.3389/fpsyt.2023.1162501
8.
Gordon, J. et al. Naturally Occurring Changes in Estradiol Concentrations in the Menopause Transition Predict Morning Cortisol and Negative Mood in Perimenopausal Depression (2016). https://doi.org/10.1177/2167702616647924
9.
Fidecicchi, T. et al. Neuroendocrine mechanisms of mood disorders during menopause transition (2024). https://doi.org/10.1016/j.maturitas.2024.108087
10.
Gava, G. et al. Cognition, Mood and Sleep in Menopausal Transition: The Role of Menopause Hormone Therapy (2019). https://doi.org/10.3390/medicina55100668
11.
Wang, D. et al. Gamma-Aminobutyric Acid Levels in the Anterior Cingulate Cortex of Perimenopausal Women With Depression: A Magnetic Resonance Spectroscopy Study (2019). https://doi.org/10.3389/fnins.2019.00785
12.
De Zambotti, M. et al. Acute stress alters autonomic modulation during sleep in women approaching menopause (2016). https://doi.org/10.1016/j.psyneuen.2015.12.017
13.
De Zambotti, M. et al. Menstrual cycle-related variation in autonomic nervous system functioning in women in the early menopausal transition with and without insomnia disorder (2016). https://doi.org/10.1016/j.psyneuen.2016.10.009
14.
Haufe, A. et al. The role of ovarian hormones in the pathophysiology of perimenopausal sleep disturbances: A systematic review (2022). https://doi.org/10.1016/j.smrv.2022.101710
15.
16.
Yu, Y. et al. Mitochondrial dysfunction in perimenopausal mood disorders: From hormonal shifts to neuroenergetic failure (2025). https://doi.org/10.3892/ijmm.2025.5656
17.
Mosconi, L. et al. Menopause impacts human brain structure, connectivity, energy metabolism, and amyloid-beta deposition (2021). https://doi.org/10.1038/s41598-021-90084-y
18.
McCarthy, M. & Raval, A. The peri-menopause in a woman’s life: a systemic inflammatory phase that enables later neurodegenerative disease (2020). https://doi.org/10.1186/s12974-020-01998-9
19.
Troìa, L. et al. Sleep Disturbance and Perimenopause: A Narrative Review (2025). https://doi.org/10.3390/jcm14051479
20.
Haufe, A. et al. The role of ovarian hormones in the pathophysiology of perimenopausal sleep disturbances: A systematic review (2022). https://doi.org/10.1016/j.smrv.2022.101710
21.
Liang, G. et al. Menopause-Associated Depression: Impact of Oxidative Stress and Neuroinflammation on the Central Nervous System: A Review (2024). https://doi.org/10.3390/biomedicines12010184
22.
Liu, M. et al. Changes in the regional homogeneity of resting-state magnetic resonance imaging in perimenopausal women (2021). https://doi.org/10.1186/s12905-020-01171-7
23.
Troìa, L. et al. Sleep Disturbance and Perimenopause: A Narrative Review (2025). https://doi.org/10.3390/jcm14051479

Mood & Energy Solutions

Fatigue Causes & Types
Fatigue Causes & Types

Workplace Strategies

Menopause at Work

Brain Fog at Work

Brain Fog at Work

Is This Perimenopause?

Is This Perimenopause?

Nutrition & Supplements

Workplace Strategies

Menopause Science

Menopause Science

Brain Fog Solutions
We use cookies and similar technologies to ensure the proper functioning of our website, personalize content, provide social media features, and analyze traffic. By clicking “I Agree”, you consent to the use of these technologies.
No results




