22 June 2026
Menopause Brain Support: Evidence-Based Ways to Protect Memory, Focus, and Cognitive Health

Reading time 17 min.

Reading time 17 min.
It is easy to lose track of whether you actually replied to an email or just thought about doing it. You are likely fighting a level of exhaustion that sleep doesn’t fix or feeling an edge of anxiety that has no obvious cause. If you are struggling with these invisible symptoms and worrying that colleagues might think you’re losing your edge, you are far from alone.
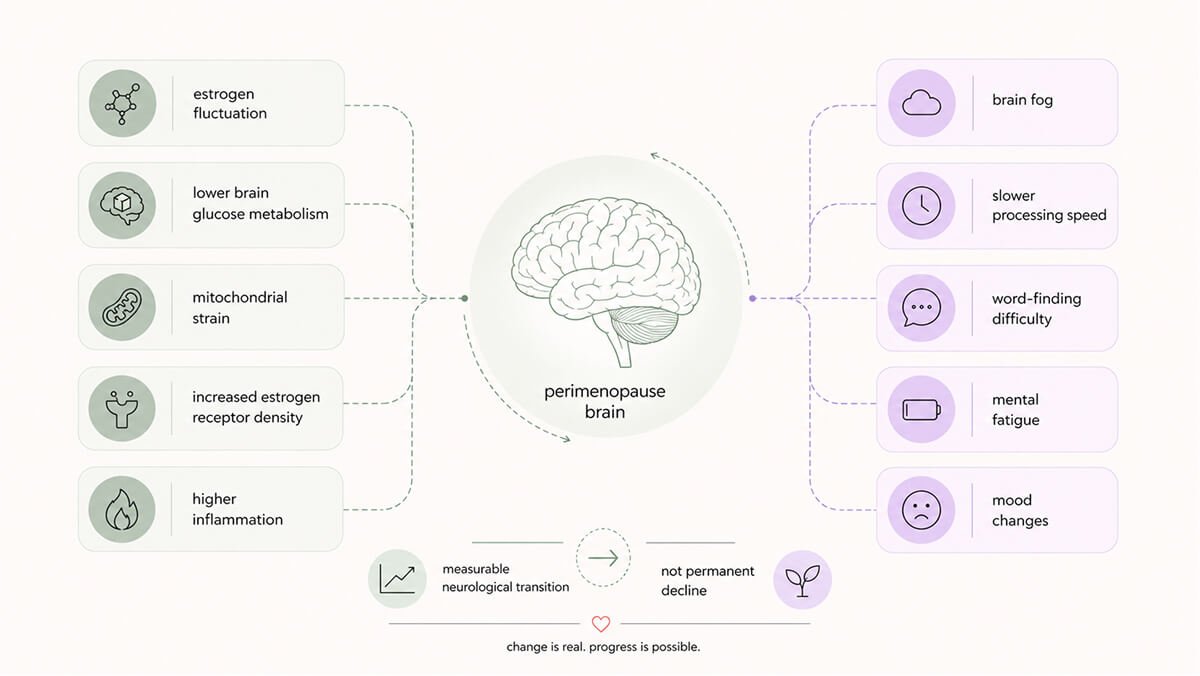
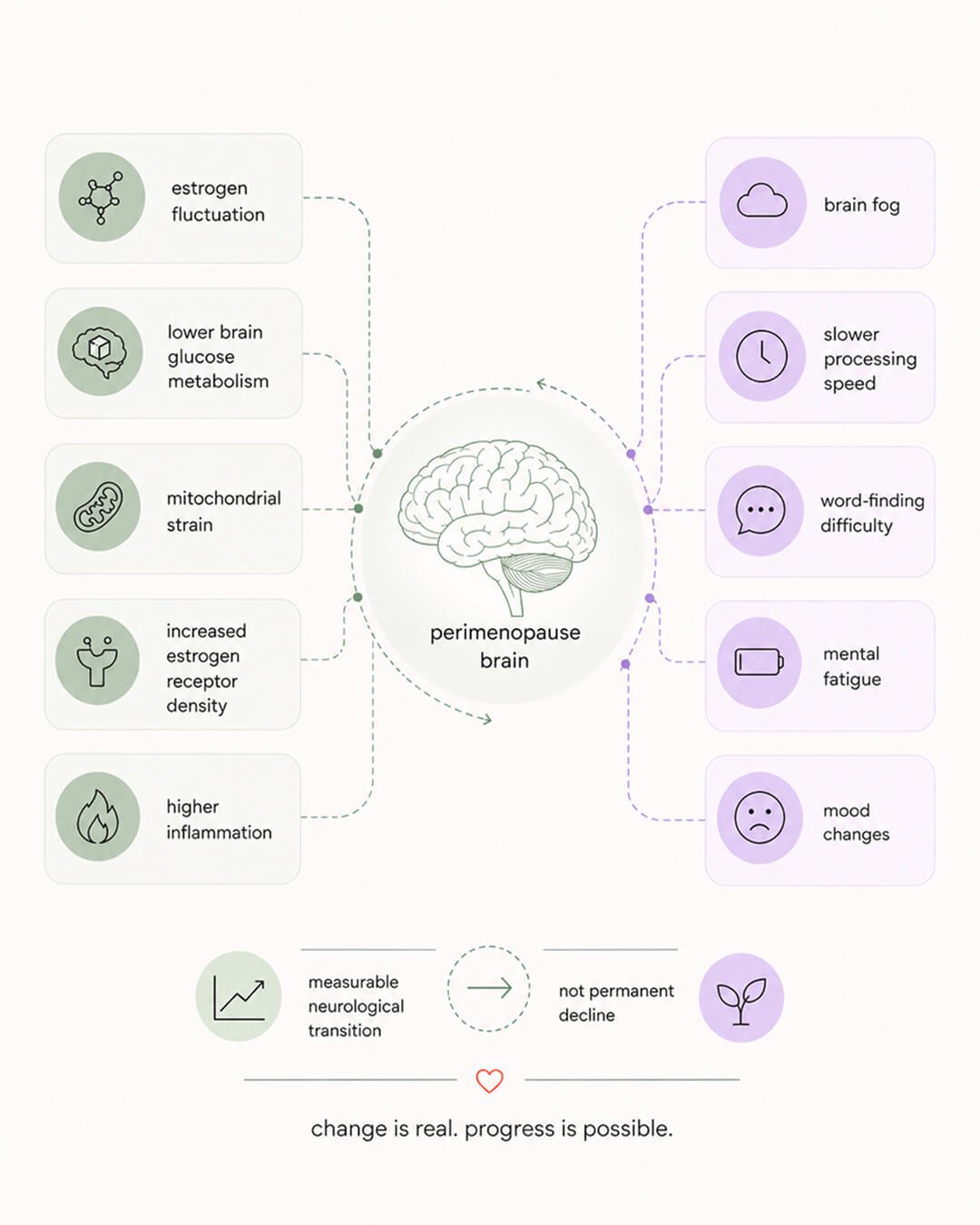
The menopause brain is moving through a real, measurable transition. Because estrogen receptors are located in every part of the brain that manages memory, focus, mood, and stress, these networks can begin to function less reliably as your hormones become unstable. The encouraging news for your long-term brain health is that support isn’t about one “miracle” fix. It is a stack of evidence-based habits, and most of them are entirely within your control.
Estrogen is not only a reproductive hormone. From your brain’s perspective, it is one of the most important regulators of how brain cells work. Estrogen helps brain cells take up glucose, keeps the energy machinery (mitochondria) inside neurons running, supports the connections between brain cells, dampens inflammation, and protects the small blood vessels that carry oxygen to your brain.1,2
When estrogen fluctuates and falls during perimenopause, every one of those functions gets disrupted at the same time. The result is what neuroscientist Roberta Brinton called a “neurological transition state,” a period when the brain is not aging on a normal curve but going through a real time restructuring.2
The clearest picture come from Mosconi’s imaging work at Weill Cornell. Brain glucose metabolism (the rate at which neurons consume glucose) drops by up to 30% in midlife women across the regions that matter most for higher-order thinking and memory: the prefrontal cortex, the hippocampus, and the posterior cingulate cortex. Age-matched men do not have the same pattern. The change is related to hormonal change.3,4
A 2024 imaging study from the same lab found something more counterintuitive. As estrogen falls, the density of estrogen receptors in the brain goes up and stays elevated in women into their mid-60s.5 Your brain is reaching harder for a signal that is no longer arriving reliably. Women with higher estrogen receptor density tended to report more mood and cognitive symptoms and performed worse on memory tests. The receptors increase as a compensation, but the compensation does not rescue the cognition.5
For most women, the metabolic restructuring resolves after postmenopause. Brain function stabilizes, sometimes at a new baseline, sometimes back to where it was before. For a smaller group, the dip continues and is associated with higher long-term risk for neurodegenerative disease.2
The cognitive changes most women notice in real time match, to a certain degree, what research finds on objective testing. The landmark SWAN data, drawn from a four-year follow-up across the menopause transition, found that perimenopausal women did not improve on tests of memory (finding your words) and processing speed (how fast you process information) the way you would expect at their age. The improvement returned after menopause.6,7 The word that does not arrive, the document you have to read twice, the sense that you are working through mud, these are predictable consequences of a brain in transition, and for most women they are temporary.
Subjective symptoms are real even when standard tests miss them. Cognitive tests used in research are blunt instruments built to detect dementia, not the kind of everyday slip a senior professional notices in herself. The gap between how you feel and what a generic test picks up is one of the most consistent patterns in the literature.8
The perimenopause brain is more sensitive to every input than it was a decade ago. Sleep, movement, food, stress, and connection were always influencing cognition. Now you feel their influence more acutely.
Two key pieces of evidence suggest that midlife is the most critical window for protecting your long-term brain health.
The first comes from the KEEPS Continuation Study, published in 2024. Researchers looked at women who had used four years of hormone therapy early in the menopause transition and re-tested them about a decade later. They found that the hormone therapy didn’t cause any long-term cognitive harm, but it didn’t offer a permanent “brain boost” either. In the end, the strongest predictor of how well a woman’s brain functioned years later was simply how well it was performing at the start. The hormone group and the placebo group ended up in the same place.9
This finding doesn’t mean hormone therapy isn’t important for other reasons. It simply suggests that, when it comes to your thinking and memory, the “cognitive cushion” you build before and during the transition is what carries you through. Deciding to use hormone therapy is a clinical choice to be made with a specialist, weighing your specific symptoms, medical history, and personal risks. Based on the current evidence, it isn’t a guaranteed strategy for preventing cognitive decline.9
The second piece of evidence comes from the 2024 Lancet Commission on Dementia Prevention. This report identified 14 manageable risk factors that, if addressed, could prevent or delay nearly half of all dementia cases worldwide. Most of these factors are most critical during midlife. Specifically, the report targets hearing loss, high cholesterol, high blood pressure, obesity, physical inactivity, diabetes, depression, and smoking as midlife priorities. Other factors, like social isolation and vision loss, become more relevant in later life, while education is a factor from our early years.10
The 45% figure is a population-wide statistic, not a personal guarantee. It represents the proportion of dementia cases across the entire population that are linked to those specific risks. It doesn’t mean that changing your habits will cut your individual risk by 45%. What it does highlight, however, is that midlife is the specific window where you have the most influence over your future brain health. The perimenopause brain is encountering these critical “levers” at the exact moment it is most responsive to them.
The transitioning perimenopause brain isn’t looking for a single “miracle” fix. Instead, the strongest evidence points toward a stack of foundational habits, each one modest on its own but powerful when they work together.
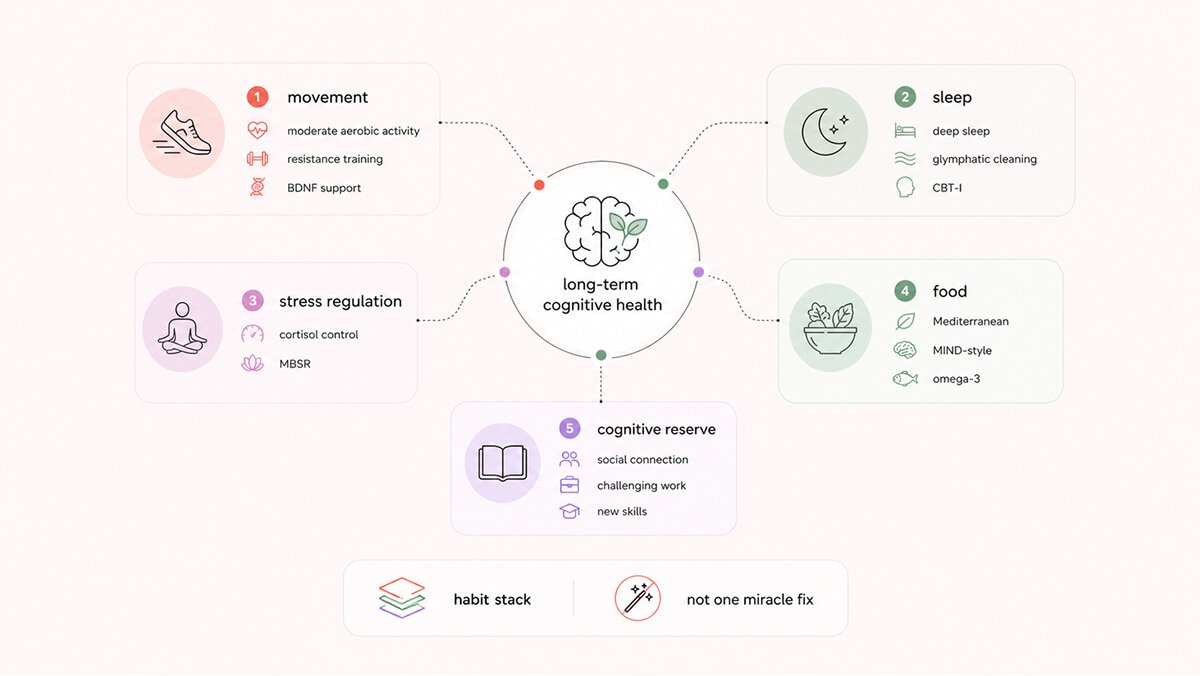

If you only had time for one thing, you would pick movement. The evidence base for exercise on midlife brain health is broader and deeper than for any other lifestyle factor.
Exercise raises brain-derived neurotrophic factor (BDNF), the protein that supports new connections between brain cells and protects existing ones. BDNF availability decreases as estrogen falls, and exercise is the most reliable way to push it back up.11,12 Older adults who walked at moderate intensity for a year actually grew their hippocampal volume, reversing the small annual shrinkage that comes with age.¹³ The hippocampus is the brain region most central to memory and one of the regions most affected by perimenopause.
Exercise does more than feed the brain. It is anti-inflammatory at the level of the brain’s immune cells (microglia), it lowers heart-disease risk factors that hit women’s cognition harder in midlife, and it improves sleep architecture, which then improves mood, attention, and the next day’s exercise capacity.14 Cardiorespiratory fitness (your ability to do sustained aerobic work) is one of the strongest known predictors of brain volume and cognitive performance across the lifespan.
The minimum effective dose of excercising is well established. The World Health Organization recommends 150 minutes per week of moderate-intensity aerobic activity, plus two sessions per week of resistance training.¹⁵ Moderate intensity means a pace where you can hold a conversation but not sing. Resistance work supports the prefrontal cortex through a separate pathway from aerobic exercise, and the two appear to add to each other.
There are two key things to understand about exercise specifically during perimenopause. First, simply sitting less is just as important as your total weekly workout time; taking short movement breaks throughout the day provides a measurable brain boost, even if you already hit the gym regularly. Second, more intensity isn’t always better. Doing too much high-intensity training can push an already stressed nervous system into a constant “fight-or-flight” state, which prevents the recovery your brain actually needs right now. Aim to keep those high-intensity sessions to just once or twice a week. Instead, build your foundation on moderate cardio and strength training.
Sleep serves as a foundation for every other health habit. Without it, your other efforts simply can’t reach their full potential.
During deep sleep, your brain activates its “waste-clearance” machinery, known as the glymphatic system. This process flushes out amyloid-beta, tau, and other metabolic byproducts that naturally accumulate during the day. When your sleep is fragmented, this cleaning process is cut short, allowing that residue to build up over time. In studies following adults from their thirties and forties for over a decade, those with the most broken-up sleep were more than twice as likely to struggle with memory and thinking later on. Crucially, it was the quality of the sleep, not just the total number of hours, that made the difference.16
Perimenopause can make a good night’s rest feel out of reach. Hot flashes and night sweats don’t just wake you up; they actively disrupt your “sleep architecture,” the natural cycle of deep and light stages your brain needs to recover. At the same time, your internal chemistry is changing. As progesterone drops, so does your supply of allopregnanolone, the brain’s built-in calming agent. Meanwhile, fluctuating estrogen destabilizes the thermostat in your hypothalamus and weakens your vagal tone. Think of vagal tone as your nervous system’s brake pedal; when it weakens, your body struggles to down-regulate and find the calm required to stay asleep.
The stress system is the other side of this same biological coin. Your primary stress response, the HPA axis, is a signaling chain that runs from your brain to your adrenal glands, releasing cortisol to help you handle pressure. In a balanced system, cortisol rises to give you energy and then signals the brain to shut the response down once the threat has passed. Estrogen and progesterone both help act as the “off switch” for this process. As these hormones become unstable during perimenopause, that switch starts to fail. It’s as if the brake on your stress response is weakening just as life starts pressing harder on the gas. Consequently, cortisol stays elevated longer, and the next stressor hits a system that hasn’t had a chance to reset.
Chronically high cortisol isn’t just an unpleasant feeling; it has physical consequences for the brain. It can shrink the hippocampus (the brain’s memory center) and hinder the growth of new brain cells. Long-term, the elevated levels are also linked to the same proteins often associated with Alzheimer’s. Keeping your stress system in check is a vital part of protecting your brain for the future.
Two interventions have the strongest evidence for the stress-sleep loop. For sleep, Cognitive Behavioral Therapy for Insomnia (CBT-I) is the first-line treatment for perimenopausal sleep problems. It outperforms sleep hygiene advice and medication, and the benefits hold long after the sessions end. Where night sweats are driving the awakenings, treating them directly is often the most efficient fix and is a conversation to have with a qualified clinician.
For stress, Mindfulness-Based Stress Reduction (MBSR) is an eight-week structured program studied in over 200 trials. In a randomized clinical trial specifically for perimenopausal women, MBSR significantly lowered stress, anxiety, and depression while improving sleep quality. The women who saw the biggest improvements were those most sensitive to hormonal shifts.¹⁷ While early brain imaging suggested that MBSR might physically change the structure of the hippocampus and amygdala, larger studies haven’t been able to prove those structural changes definitively.18,19 However, the functional benefits are much more reliable: the practice consistently lowers cortisol levels and helps the nervous system regulate itself more effectively. For a brain in transition, that ability to “reset” the stress response is a major win.
The remaining foundations look like ordinary life rather than treatment, which is why they get underestimated.
Two dietary patterns have the strongest evidence for protecting the aging brain. The Mediterranean diet is built on vegetables, legumes, whole grains, olive oil, fish, nuts, and modest amounts of dairy and red meat. The MIND diet (Mediterranean-DASH Intervention for Neurodegenerative Delay) is a brain-focused diet refinement that emphasizes leafy greens, berries, nuts, beans, whole grains, fish, and olive oil. Higher adherence to either pattern is associated with slower cognitive decline and lower dementia risk in multiple large studies.20,21 The longest follow-ups suggest the MIND diet may have a slight edge for cognitive outcomes specifically, though the evidence varies across populations.21
The mechanism is not mysterious. Both patterns deliver omega-3 fats, polyphenols, B vitamins, fiber, and antioxidants while keeping processed foods, added sugars, and trans fats low. They support the gut microbiome, reduce systemic inflammation, and lower heart-disease risk, all of which feed back into brain health.
Your brain is roughly 60% fat by dry weight, and DHA is the primary structural fat in neuronal membranes. Estrogen helps maintain DHA levels in the body, so as estrogen declines, the risk of low DHA increases. Midlife adults with higher red blood cell omega-3 levels had larger hippocampal volumes and better abstract reasoning as it was shown in the Framingham Heart Study.22 Two servings per week of oily fish (salmon, mackerel, sardines, herring) are sufficient for most women. Supplementation makes sense where dietary intake is genuinely low.
A 2025 analysis used advanced modeling on data from 30,000 older adults and 137,000 cognitive tests to look at the link between social life and brain health. The study found that social isolation, measured by how much you actually interact with others, directly speeds up cognitive decline. Interestingly, this happened regardless of whether the person actually felt lonely.23 Loneliness and isolation are not the same thing; the data shows that the measurable lack of interaction is what drives the damage to the brain.
The reason is straightforward. Engaging with other people, particularly those outside your immediate circle, is a high-level workout for your brain. It forces you to use memory, language, attention, and emotional control all at once. Very few daily activities challenge that many different neural networks at the same time. Maintaining these social connections is a powerful, active way to keep your brain sharp.
Cognitive reserve is the biological cushion that determines how well your brain handles aging. It explains why two people can have the same physical signs of aging in their brains, yet one remains sharp for years while the other struggles with dementia. The difference is the “backup capacity” your brain has built up.
You build this reserve throughout your life through education, a challenging career, and staying mentally active. The good news is that it’s never too late to add to it. Research shows that engaging in social and intellectually stimulating activities during midlife builds your brain’s resilience regardless of your earlier education or job title.24,25 However, the key is to challenge yourself: learning genuinely new skills, the kind that feel difficult and a little uncomfortable, builds this protective cushion in a way that simply practicing things you’re already good at does not.
This brings us back to the KEEPS Continuation Study. The strongest predictor of where your memory and thinking will be ten years from now is where they are today. Your cognitive reserve is the infrastructure that protects you, and midlife is the most critical time to strengthen it.
The perimenopause brain is not failing. It is moving through a significant biological transition, and the path it takes from here is something you can actively shape. Supporting your brain during this time isn’t about finding one “miracle” fix; it’s about building a solid foundation.
Regular movement, quality sleep, a Mediterranean or MIND-style diet, and staying socially connected to people who truly challenge your intelligence all play a role. When you combine these with deliberate stress management, the benefits compound. The strongest predictor of where your memory and focus will be in ten years is where they are today. What you do during this transition matters far more than what you do later. Your brain is resilient and responsive; it’s ready to work with you.
Dr. Jura Lasas
1.
Mosconi, L. et al. Perimenopause and emergence of an Alzheimer’s bioenergetic phenotype in brain and periphery (2017). https://doi.org/10.1371/journal.pone.0185926
2.
Brinton, R. D. et al. Perimenopause as a neurological transition state (2015). https://doi.org/10.1038/nrendo.2015.82
3.
Mosconi, L. et al. Sex differences in Alzheimer risk: Brain imaging of endocrine vs chronologic aging (2017). https://doi.org/10.1212/WNL.0000000000004425
4.
Mosconi, L. et al. Menopause impacts human brain structure, connectivity, energy metabolism, and amyloid-beta deposition (2021). https://doi.org/10.1038/s41598-021-90084-y
5.
Mosconi, L. et al. In vivo brain estrogen receptor density by neuroendocrine aging and relationships with cognition and symptomatology (2024). https://doi.org/10.1038/s41598-024-62820-7
6.
Greendale, G. A. et al. Effects of the menopause transition and hormone use on cognitive performance in midlife women (2009). https://doi.org/10.1212/WNL.0b013e3181a71193
7.
Weber, M. T. et al. Cognition and mood in perimenopause: A systematic review and meta-analysis (2014). https://doi.org/10.1016/j.jsbmb.2013.06.001
8.
Maki, P. M. & Jaff, N. G. Brain fog in menopause: a health-care professional’s guide for decision-making and counseling on cognition (2022). https://doi.org/10.1080/13697137.2022.2122792
9.
Gleason, C. E. et al. Long-term cognitive effects of menopausal hormone therapy: Findings from the KEEPS Continuation Study (2024). https://doi.org/10.1371/journal.pmed.1004435
10.
Livingston, G. et al. Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission (2024). https://doi.org/10.1016/S0140-6736(24)01296-0
11.
Pareja-Galeano, H. et al. Exercise as a polypill for chronic diseases (2015). https://doi.org/10.1016/bs.pmbts.2015.07.019
12.
Wang, Y. et al. The effect of physical exercise on circulating brain-derived neurotrophic factor in healthy subjects: A meta-analysis of randomized controlled trials (2022). https://doi.org/10.1002/brb3.2544
13.
Erickson, K. I. et al. Exercise training increases size of hippocampus and improves memory (2011). https://doi.org/10.1073/pnas.1015950108
14.
Northey, J. M. et al. Exercise interventions for cognitive function in adults older than 50: a systematic review with meta-analysis (2018). https://doi.org/10.1136/bjsports-2016-096587
15.
Bull, F. C. et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour (2020). https://doi.org/10.1136/bjsports-2020-102955
16.
Leng, Y. et al. Objective sleep characteristics and cognitive performance in midlife: A 11-year follow-up study of the CARDIA cohort (2024). https://doi.org/10.1212/WNL.0000000000208056
17.
Gordon, J. L. et al. Endocrine and psychosocial moderators of mindfulness-based stress reduction for the prevention of perimenopausal depressive symptoms: A randomized controlled trial (2021). https://doi.org/10.1016/j.psyneuen.2021.105277
18.
Hölzel, B. K. et al. Mindfulness practice leads to increases in regional brain gray matter density (2011). https://doi.org/10.1016/j.pscychresns.2010.08.006
19.
Kral, T. R. A. et al. Absence of structural brain changes from mindfulness-based stress reduction: Two combined randomized controlled trials (2022). https://doi.org/10.1126/sciadv.abk3316
20.
van den Brink, A. C. et al. The Mediterranean, DASH, and MIND diets are associated with less cognitive decline and a lower risk of Alzheimer’s disease (2019). https://doi.org/10.3945/an.118.012116
21.
Agarwal, P. et al. Association of MIND diet with cognitive decline among Black and White older adults (2024). https://doi.org/10.1002/alz.14277
22.
Satizabal, C. L. et al. Association of red blood cell omega-3 fatty acids with MRI markers and cognitive function in midlife: The Framingham Heart Study (2022). https://doi.org/10.1212/WNL.0000000000201296
23.
Hale, J. M. et al. Disentangling social isolation, loneliness, and later-life cognitive function for older adults in the United States: Evidence from causal inference modeling (2025). https://doi.org/10.1093/geronb/gbaf254
24.
Chan, D. et al. Lifestyle activities in mid-life contribute to cognitive reserve in late-life, independent of education, occupation and late-life activities (2018). https://doi.org/10.1016/j.neurobiolaging.2018.05.018
25.
Livingston, G. et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission (2020). https://doi.org/10.1016/S0140-6736(20)30367-6

Mood & Energy Solutions

Fatigue Causes & Types
Fatigue Causes & Types

Workplace Strategies

Menopause at Work

Brain Fog at Work

Brain Fog at Work

Is This Perimenopause?

Is This Perimenopause?

Nutrition & Supplements

Workplace Strategies

Menopause Science

Menopause Science

Brain Fog Solutions
We use cookies and similar technologies to ensure the proper functioning of our website, personalize content, provide social media features, and analyze traffic. By clicking “I Agree”, you consent to the use of these technologies.
No results




